Zahedi Maryam, Asghari Golaleh, Mirmiran Parvin, Hosseinpanah Farhad
Obesity Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Nutrition and Endocrine Research Center, Research Institute for Endocrine Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Front Nutr. 2021 Mar 5;8:602938. doi: 10.3389/fnut.2021.602938. eCollection 2021.
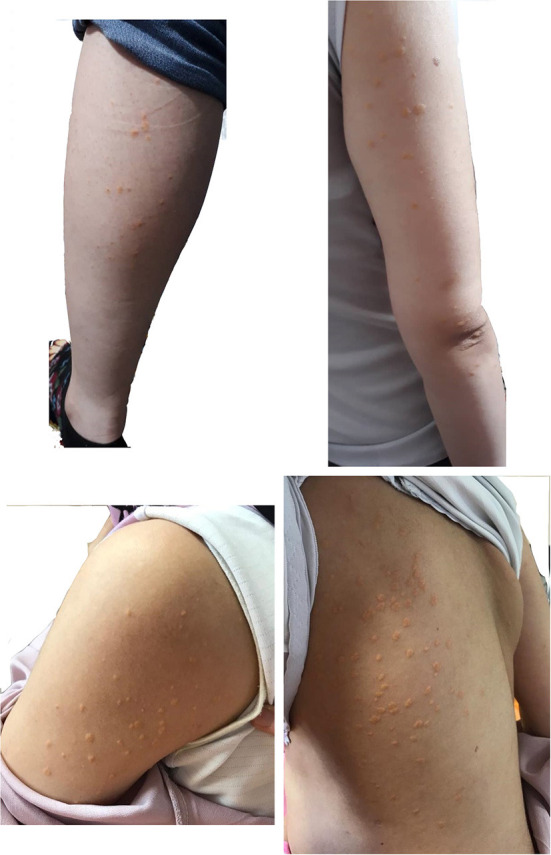
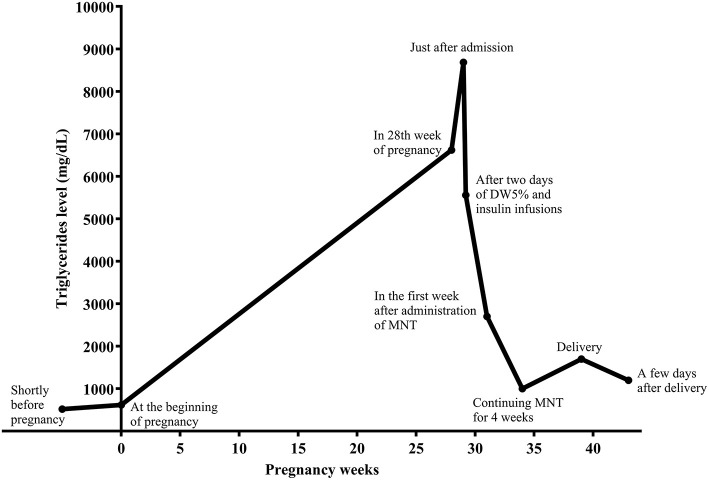
Hypertriglyceridemia (HTG) during pregnancy may be accompanied by acute pancreatitis, hyperviscosity syndrome, and preeclampsia. HTG during pregnancy should be managed by a multidisciplinary team; however, no clinical guidelines exist for severe gestational HTG. We herein present a case of a 36-year-old in the first pregnancy (G1P0Ab0), with a history of severe HTG-induced necrotizing pancreatitis 9 years earlier. There was no family history of HTG. During these years, she did not follow any appropriate diet or medical therapy for HTG. She became pregnant in May 2019, without preconception counseling. Eruptive and tuberoeruptive xanthomas appeared in the 27th week of pregnancy. Serum triglycerides (TGs) and fasting blood sugar (FBS) were 6,620 and 124 mg/dL, respectively, indicating HTG and gestational diabetes (GDM). After admission for the management of severe HTG, she was put on parenteral nutrition with dextrose water 5% and infusion insulin therapy without receiving any enteral carbohydrate for 2 days. Following that, a very low-fat diet and omega-3 fatty acids (1,200 mg/day) were started. After 4 weeks, TG levels reached 1,000 mg/dL, and her self-monitoring blood glucose levels showed appropriate blood glucose for pregnancy. She underwent a successful elective cesarean section in the 39th of pregnancy. This case report demonstrates that HTG during pregnancy could be managed by medical nutrition therapy (MNT).
孕期高甘油三酯血症(HTG)可能伴有急性胰腺炎、高黏滞综合征和子痫前期。孕期HTG应由多学科团队管理;然而,目前尚无针对重度妊娠HTG的临床指南。我们在此报告一例36岁初产妇(G1P0Ab0),9年前有重度HTG诱发坏死性胰腺炎病史。无HTG家族史。这些年里,她未遵循任何针对HTG的适当饮食或药物治疗。2019年5月她怀孕,未进行孕前咨询。孕27周时出现疹性和结节疹性黄瘤。血清甘油三酯(TGs)和空腹血糖(FBS)分别为6620和124mg/dL,提示HTG和妊娠期糖尿病(GDM)。因重度HTG入院治疗后,她接受了2天的5%葡萄糖水肠外营养和静脉输注胰岛素治疗,未摄入任何肠内碳水化合物。此后,开始采用极低脂肪饮食和ω-3脂肪酸(1200mg/天)。4周后,TG水平降至1000mg/dL,她的自我血糖监测显示血糖水平适合孕期。孕39周时她成功接受了择期剖宫产。本病例报告表明,孕期HTG可通过医学营养治疗(MNT)进行管理。