Takahashi Norihito, Dohi Tomotaka, Endo Hirohisa, Takeuchi Mitsuhiro, Doi Shinichiro, Kato Yoshiteru, Okai Iwao, Iwata Hiroshi, Okazaki Shinya, Isoda Kikuo, Miyauchi Katsumi, Minamino Tohru
Department of Cardiovascular Biology and Medicine, Juntendo University Graduate School of Medicine, 2-1-1 Hongo, Bunkyo-ku, Tokyo 113-0033, Japan.
Japan Agency for Medical Research and Development Core Research for Evolutionary Medical Science and Technology (AMEDCREST), Japan Agency for Medical Research and Development, 1-7-1 Otemachi, Chiyoda-ku, Tokyo, Japan.
Int J Cardiol Heart Vasc. 2021 Mar 11;33:100747. doi: 10.1016/j.ijcha.2021.100747. eCollection 2021 Apr.
Asians have a much lower incidence of adverse coronary events than Caucasians. We sought to evaluate the characteristics of coronary lipid-rich plaques (LRP) in Asian patients with acute coronary syndrome (ACS) and stable angina (SA). We also aimed to identify surrogate markers for the extent of LRP.
We evaluated 207 patients (ACS, n = 75; SA, n = 132) who underwent percutaneous coronary intervention under near infrared spectroscopy intravascular ultrasound (NIRS-IVUS). Plaque characteristics and the extent of LRP [defined as a long segment with a 4-mm maximum lipid-core burden index (maxLCBI)] on NIRS in de-novo culprit and non-culprit segments were analyzed.
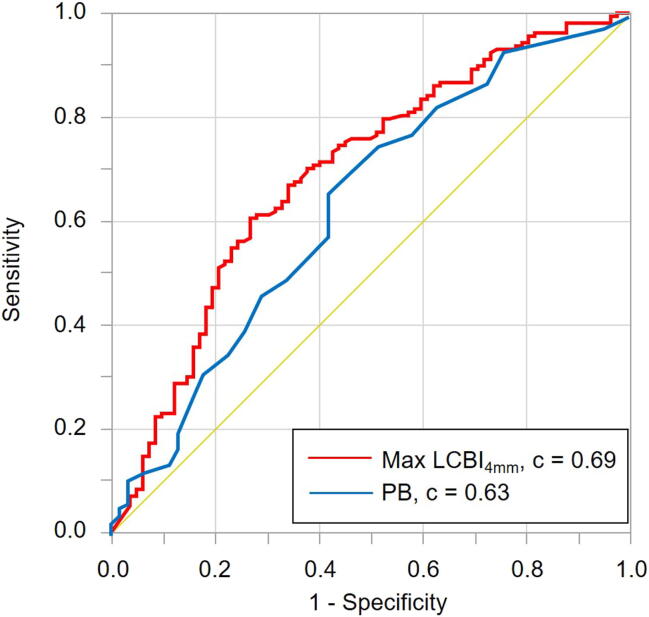
The ACS culprit lesions had a significantly higher maxLCBI (median [interquartile range (IQR)]: 533 [385-745] vs. 361 [174-527], < 0.001) than the SA culprit lesions. On multivariate logistic analysis, a large LRP (defined as maxLCBI ≥ 400) was the strongest independent predictor of the ACS culprit segment (odds ratio, 3.87; 95% confidence interval, 1.95-8.02). In non-culprit segments, 19.8% of patients had at least one large LRP without a small lumen. No significant correlation was found between the extent of LRP and systematic biomarkers (hs-CRP, IL-6, TNF-α), whereas the extent of LRP was positively correlated with IVUS plaque burden (r = 0.24, < 0.001).
We confirmed that NIRS-IVUS plaque assessment could be useful to differentiate ACS from SA culprit lesions, and that a threshold maxLCBI ≥ 400 was clinically suitable in Japanese patients. No surrogate maker for a high-risk LRP was found; consequently, direct intravascular evaluation of plaque characteristics remains important.
亚洲人发生不良冠状动脉事件的发生率远低于白种人。我们试图评估亚洲急性冠状动脉综合征(ACS)和稳定型心绞痛(SA)患者冠状动脉富含脂质斑块(LRP)的特征。我们还旨在确定LRP范围的替代标志物。
我们评估了207例接受近红外光谱血管内超声(NIRS-IVUS)引导下经皮冠状动脉介入治疗的患者(ACS患者75例,SA患者132例)。分析了初发罪犯病变和非罪犯病变节段的斑块特征以及NIRS上LRP的范围[定义为最大脂质核心负担指数(maxLCBI)为4 mm的长节段]。
ACS罪犯病变的maxLCBI显著高于SA罪犯病变(中位数[四分位间距(IQR)]:533[385 - 745]对361[174 - 527],<0.001)。多因素逻辑分析显示,大LRP(定义为maxLCBI≥400)是ACS罪犯节段最强的独立预测因子(比值比,3.87;95%置信区间,1.95 - 8.02)。在非罪犯节段,19.8%的患者至少有一个无小腔的大LRP。LRP范围与系统性生物标志物(hs-CRP、IL-6、TNF-α)之间未发现显著相关性,而LRP范围与IVUS斑块负荷呈正相关(r = 0.24,<0.001)。
我们证实NIRS-IVUS斑块评估有助于区分ACS和SA罪犯病变,并且maxLCBI≥400的阈值在日本患者中临床适用。未发现高危LRP的替代标志物;因此,直接血管内评估斑块特征仍然很重要。