Lancet Elizabeth A, Gonzalez Dario, Alexandrou Nikolaos A, Zabar Benjamin, Lai Pamela H, Hall Charles B, Braun James, Zeig-Owens Rachel, Isaacs Douglas, Ben-Eli David, Reisman Nathan, Kaufman Bradley, Asaeda Glenn, Weiden Michael D, Nolan Anna, Teo Hugo, Wei Eric, Natsui Shaw, Philippou Christopher, Prezant David J
Office of Medical Affairs Fire Department of the City of New York Brooklyn New York USA.
Department of Epidemiology and Population Health Albert Einstein College of Medicine Bronx New York USA.
J Am Coll Emerg Physicians Open. 2021 Mar 17;2(2):e12407. doi: 10.1002/emp2.12407. eCollection 2021 Apr.
To determine if oxygen saturation (out-of-hospital SpO2), measured by New York City (NYC) 9-1-1 Emergency Medical Services (EMS), was an independent predictor of coronavirus disease 2019 (COVID-19) in-hospital mortality and length of stay, after controlling for the competing risk of death. If so, out-of-hospital SpO2 could be useful for initial triage.
A population-based longitudinal study of adult patients transported by EMS to emergency departments (ED) between March 5 and April 30, 2020 (the NYC COVID-19 peak period). Inclusion required EMS prehospital SpO2 measurement while breathing room air, transport to emergency department, and a positive severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) reverse transcription polymerase chain reaction test. Multivariable logistic regression modeled mortality as a function of prehospital SpO2, controlling for covariates (age, sex, race/ethnicity, and comorbidities). A competing risk model also was performed to estimate the absolute risks of out-of-hospital SpO2 on the cumulative incidence of being discharged from the hospital alive.
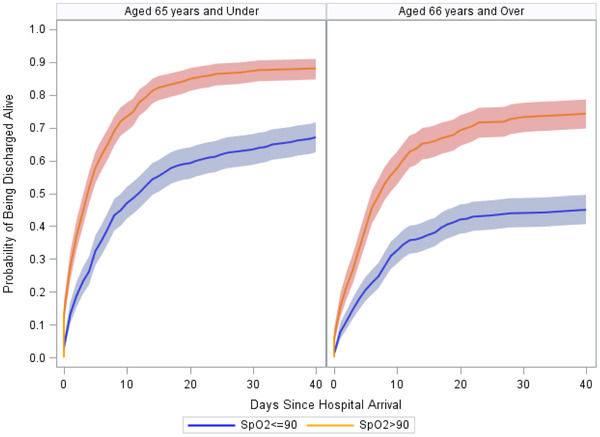
In 1673 patients, out-of-hospital SpO2 and age were independent predictors of in-hospital mortality and length of stay, after controlling for the competing risk of death. Among patients ≥66 years old, the probability of death was 26% with an out-of-hospital SpO2 >90% versus 54% with an out-of-hospital SpO2 ≤90%. Among patients <66 years old, the probability of death was 11.5% with an out-of-hospital SpO2 >90% versus 31% with an out-of-hospital SpO2 ≤ 90%. An out-of-hospital SpO2 level ≤90% was associated with over 50% decreased likelihood of being discharged alive, regardless of age.
Out-of-hospital SpO2 and age predicted in-hospital mortality and length of stay: An out-of-hospital SpO2 ≤90% strongly supports a triage decision for immediate hospital admission. For out-of-hospital SpO2 >90%, the decision to admit depends on multiple factors, including age, resource availability (outpatient vs inpatient), and the potential impact of new treatments.
在控制死亡这一竞争风险后,确定由纽约市(NYC)9-1-1紧急医疗服务(EMS)测量的血氧饱和度(院外SpO2)是否为2019冠状病毒病(COVID-19)院内死亡率和住院时间的独立预测因素。如果是,院外SpO2可能有助于初始分诊。
对2020年3月5日至4月30日期间(NYC COVID-19高峰期)由EMS转运至急诊科(ED)的成年患者进行一项基于人群的纵向研究。纳入标准要求在呼吸室内空气时进行EMS院前SpO2测量、转运至急诊科以及严重急性呼吸综合征冠状病毒2(SARS-CoV-2)逆转录聚合酶链反应检测呈阳性。多变量逻辑回归将死亡率建模为院前SpO2的函数,并控制协变量(年龄、性别、种族/民族和合并症)。还进行了一个竞争风险模型,以估计院外SpO2对存活出院累积发生率的绝对风险。
在1673例患者中,在控制死亡这一竞争风险后,院外SpO2和年龄是院内死亡率和住院时间的独立预测因素。在≥66岁的患者中,院外SpO2>90%时死亡概率为26%,而院外SpO2≤90%时为54%。在<66岁的患者中,院外SpO2>90%时死亡概率为11.5%,而院外SpO2≤90%时为31%。无论年龄如何,院外SpO2水平≤90%与存活出院可能性降低超过50%相关。
院外SpO2和年龄可预测院内死亡率和住院时间:院外SpO2≤90%有力支持立即住院的分诊决定。对于院外SpO2>90%的情况,入院决定取决于多种因素,包括年龄、资源可用性(门诊与住院)以及新治疗方法的潜在影响。