Makerere University-Johns Hopkins University (MU-JHU) Research Collaboration, Upper Mulago Hill Road, Mulago, P.O.BOX 23491, Kampala, Uganda.
Nsambya Home Care Project (NHC), Kampala, Uganda.
BMC Pediatr. 2021 Mar 22;21(1):139. doi: 10.1186/s12887-021-02608-0.
Many HIV-infected African children gained access to antiretroviral treatment (ART) through expansion of PEPFAR programs since 2004 and introduction of "Test and Treat" WHO guidelines in 2015. As ART access increases and children transition from adolescence to adulthood, treatment failure is inevitable. Viral load (VL) monitoring in Uganda was introduced in 2016 replacing clinical monitoring. However, there's limited data on the comparative effectiveness of these two strategies among HIV-infected children in resource-limited settings (RLS).
HIV-infected Ugandan children aged 1-12 years from HIV-care programs with > 1 year of first-line ART using only immunologic and clinical criteria to monitor response to treatment were screened in 2010. Eligible children were stratified by VL ≤ 400 and > 400 copies/ml randomized to clinical and immunological (control) versus clinical, immunological and VL monitoring to determine treatment failure with follow-up at 12, 24, 36, and 48 weeks. Plasma VL was analyzed retrospectively for controls. Mixed-effects logistic regression models were used to compare the prevalence of viral suppression between study arms and identify factors associated with viral suppression.
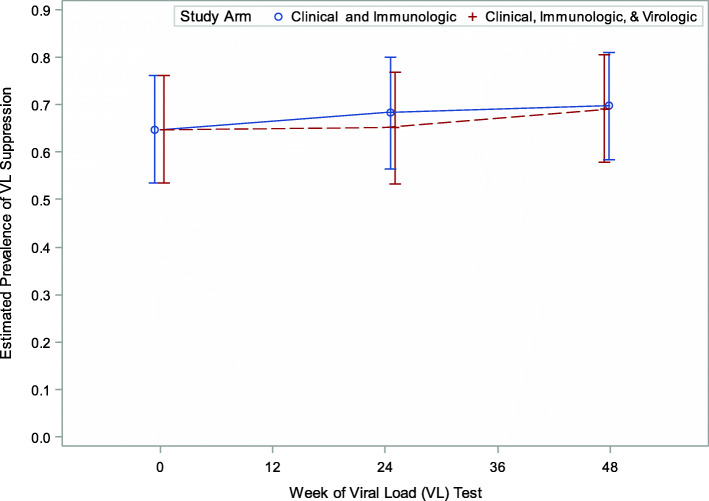
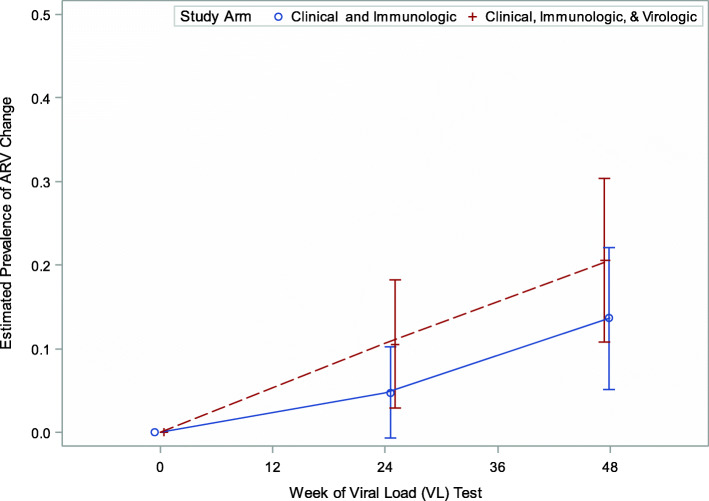
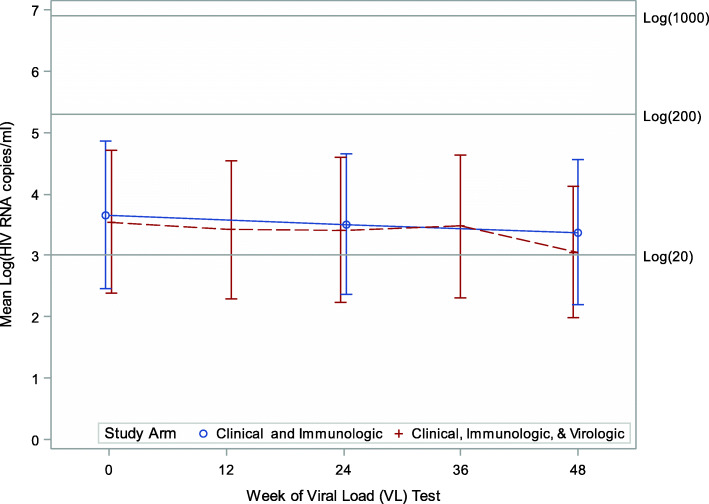
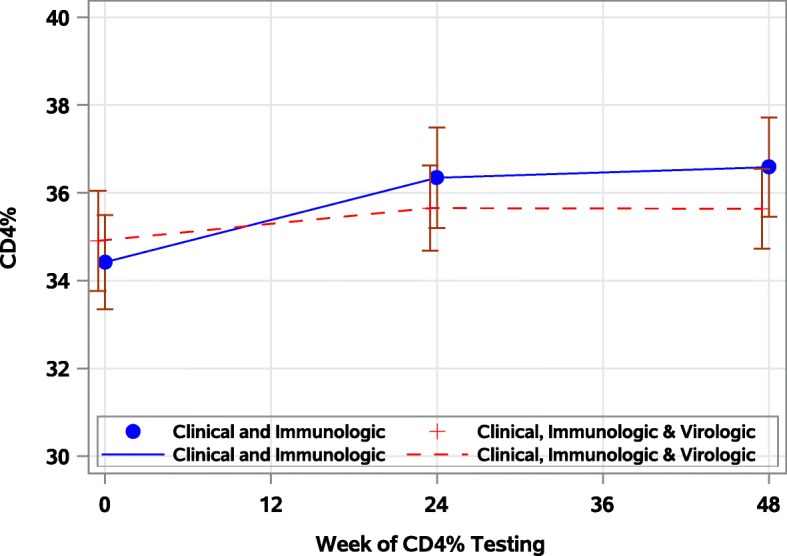
At baseline all children (n = 142) were on NNRTI based ART (75% Nevirapine, 25% efavirenz). One third of ART-experienced children had detectable VL at baseline despite high CD4%. Median age was 6 years (interquartile range [IQR]: 5-9) and 43% were female. Overall, the odds of viral suppression were not different between study arms: (arm by week interaction, p = 0.63), adjusted odds ratio [aOR]: 1.07; 95%CI: 0.53, 2.17, p = 0.57) and did not change over time (aOR: 0 vs 24 week: 1.15; 95% CI: 0.91, 1.46, p = 0.24 and 0 vs 48 weeks: 1.26; 95%CI: 0.92, 1.74, p = 0.15). Longer duration of a child's ART exposure was associated with lower odds of viral suppression (aOR: 0.61; 95% CI: 0.42, 0.87, p < .01). Only 13% (9/71) of children with virologic failure were switched to second-line ART, in spite of access to real-time VL.
With increasing ART exposure, viral load monitoring is critical for early detection of treatment failure in RLS. Clinicians need to make timely informed decisions to switch failing children to second-line ART.
ClinicalTrials.gov NCT04489953 , 28 Jul 2020. Retrospectively registered. ( https://register.clinicaltrials.gov ).
自 2004 年以来,通过扩大美国国际开发署(PEPFAR)计划,许多感染艾滋病毒的非洲儿童获得了抗逆转录病毒治疗(ART),并且在 2015 年引入了世卫组织“检测即治疗”指南。随着 ART 机会的增加,儿童从青少年过渡到成年,治疗失败是不可避免的。乌干达于 2016 年引入了病毒载量(VL)监测,取代了临床监测。然而,在资源有限的环境中(RLS),针对 HIV 感染儿童,这两种策略的相对有效性的数据有限。
2010 年,对接受一线 ART 治疗超过 1 年的、仅使用免疫和临床标准监测治疗反应的 1-12 岁感染艾滋病毒的乌干达儿童艾滋病毒护理项目进行了筛查。根据 VL≤400 和>400 拷贝/ml 对符合条件的儿童进行分层,随机分配至临床和免疫(对照组)与临床、免疫和 VL 监测,以确定治疗失败,并在 12、24、36 和 48 周进行随访。对对照组进行回顾性血浆 VL 分析。使用混合效应逻辑回归模型比较研究臂之间病毒抑制的发生率,并确定与病毒抑制相关的因素。
在基线时(n=142),所有儿童均接受基于 NNRTI 的 ART(75%奈韦拉平,25%依非韦伦)治疗。尽管 CD4%较高,但三分之一的 ART 经验丰富的儿童基线时仍可检测到 VL。中位年龄为 6 岁(四分位距[IQR]:5-9),43%为女性。总体而言,研究臂之间病毒抑制的几率没有差异:(臂与周的交互作用,p=0.63),调整后的优势比[aOR]:1.07;95%CI:0.53,2.17,p=0.57),且随时间变化无变化(aOR:0 与 24 周:1.15;95%CI:0.91,1.46,p=0.24 和 0 与 48 周:1.26;95%CI:0.92,1.74,p=0.15)。儿童接受 ART 治疗的时间越长,病毒抑制的几率越低(aOR:0.61;95%CI:0.42,0.87,p<0.01)。尽管可以获得实时 VL,但只有 13%(9/71)的病毒学失败儿童被转换为二线 ART。
随着 ART 暴露的增加,病毒载量监测对于 RLS 中治疗失败的早期检测至关重要。临床医生需要及时做出明智的决策,将失败的儿童转用二线 ART。
ClinicalTrials.gov NCT04489953,2020 年 7 月 28 日。回顾性注册。(https://register.clinicaltrials.gov)。