Szubert Alexander J, Prendergast Andrew J, Spyer Moira J, Musiime Victor, Musoke Philippa, Bwakura-Dangarembizi Mutsa, Nahirya-Ntege Patricia, Thomason Margaret J, Ndashimye Emmanuel, Nkanya Immaculate, Senfuma Oscar, Mudenge Boniface, Klein Nigel, Gibb Diana M, Walker A Sarah
MRC Clinical Trials Unit at University College London, London, United Kingdom.
Queen Mary University of London, London, United Kingdom.
PLoS Med. 2017 Nov 14;14(11):e1002432. doi: 10.1371/journal.pmed.1002432. eCollection 2017 Nov.
Although WHO recommends viral load (VL) monitoring for those on antiretroviral therapy (ART), availability in low-income countries remains limited. We investigated long-term VL and resistance in HIV-infected children managed without real-time VL monitoring.
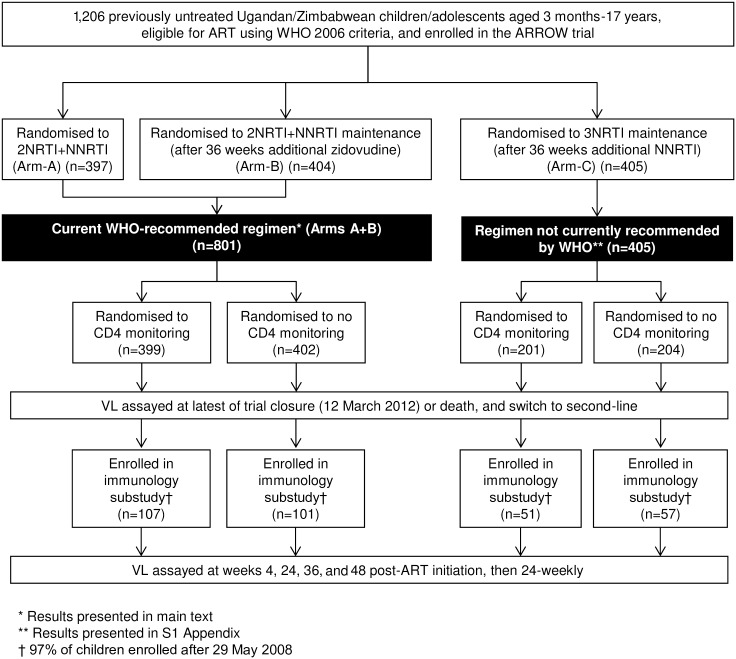
In the ARROW factorial trial, 1,206 children initiating ART in Uganda and Zimbabwe between 15 March 2007 and 18 November 2008, aged a median 6 years old, with median CD4% of 12%, were randomised to monitoring with or without 12-weekly CD4 counts and to receive 2 nucleoside reverse transcriptase inhibitors (2NRTI, mainly abacavir+lamivudine) with a non-nucleoside reverse transcriptase inhibitor (NNRTI) or 3 NRTIs as long-term ART. All children had VL assayed retrospectively after a median of 4 years on ART; those with >1,000 copies/ml were genotyped. Three hundred and sixteen children had VL and genotypes assayed longitudinally (at least every 24 weeks). Overall, 67 (6%) switched to second-line ART and 54 (4%) died. In children randomised to WHO-recommended 2NRTI+NNRTI long-term ART, 308/378 (81%) monitored with CD4 counts versus 297/375 (79%) without had VL <1,000 copies/ml at 4 years (difference = +2.3% [95% CI -3.4% to +8.0%]; P = 0.43), with no evidence of differences in intermediate/high-level resistance to 11 drugs. Among children with longitudinal VLs, only 5% of child-time post-week 24 was spent with persistent low-level viraemia (80-5,000 copies/ml) and 10% with VL rebound ≥5,000 copies/ml. No child resuppressed <80 copies/ml after confirmed VL rebound ≥5,000 copies/ml. A median of 1.0 (IQR 0.0,1.5) additional NRTI mutation accumulated over 2 years' rebound. Nineteen out of 48 (40%) VLs 1,000-5,000 copies/ml were immediately followed by resuppression <1,000 copies/ml, but only 17/155 (11%) VLs ≥5,000 copies/ml resuppressed (P < 0.0001). Main study limitations are that analyses were exploratory and treatment initiation used 2006 criteria, without pre-ART genotypes.
In this study, children receiving first-line ART in sub-Saharan Africa without real-time VL monitoring had good virological and resistance outcomes over 4 years, regardless of CD4 monitoring strategy. Many children with detectable low-level viraemia spontaneously resuppressed, highlighting the importance of confirming virological failure before switching to second-line therapy. Children experiencing rebound ≥5,000 copies/ml were much less likely to resuppress, but NRTI resistance increased only slowly. These results are relevant to the increasing numbers of HIV-infected children receiving first-line ART in sub-Saharan Africa with limited access to virological monitoring.
ISRCTN Registry, ISRCTN24791884.
尽管世界卫生组织建议对接受抗逆转录病毒治疗(ART)的患者进行病毒载量(VL)监测,但在低收入国家,这种监测的可及性仍然有限。我们调查了在没有实时VL监测的情况下接受管理的HIV感染儿童的长期VL和耐药情况。
在ARROW析因试验中,2007年3月15日至2008年11月18日期间,乌干达和津巴布韦的1206名开始接受ART的儿童被随机分组,这些儿童年龄中位数为6岁,CD4%中位数为12%,被随机分配接受每12周一次的CD4计数监测或不接受该监测,并接受2种核苷类逆转录酶抑制剂(2NRTI,主要是阿巴卡韦+拉米夫定)加一种非核苷类逆转录酶抑制剂(NNRTI)或3种NRTI作为长期ART治疗。所有儿童在接受ART治疗中位数4年后进行回顾性VL检测;VL>1000拷贝/毫升的儿童进行基因分型。316名儿童进行了纵向VL和基因型检测(至少每24周一次)。总体而言,67名(6%)儿童改用二线ART,54名(4%)儿童死亡。在随机接受世界卫生组织推荐的2NRTI+NNRTI长期ART治疗的儿童中,接受CD4计数监测的308/378名(81%)儿童与未接受该监测的297/375名(79%)儿童在4年时VL<1000拷贝/毫升(差异=+2.3%[95%CI -3.4%至+8.0%];P=0.43),没有证据表明对11种药物的中/高水平耐药存在差异。在进行纵向VL检测的儿童中,在第24周后的儿童时间里,只有5%的时间处于持续低水平病毒血症(80 - 5000拷贝/毫升),10%的时间VL反弹≥5000拷贝/毫升。在确认VL反弹≥5000拷贝/毫升后,没有儿童重新抑制到<80拷贝/毫升。在2年的反弹期间,平均额外积累了1.0(IQR 0.0,1.5)个NRTI突变。48名VL为1000 - 5000拷贝/毫升的儿童中有19名(40%)随后立即重新抑制到<1000拷贝/毫升,但VL≥5000拷贝/毫升的儿童中只有17/155名(11%)重新抑制(P<0.0001)。主要研究局限性在于分析是探索性的,且治疗开始采用的是2006年标准且没有ART前的基因型。
在本研究中,撒哈拉以南非洲地区在没有实时VL监测的情况下接受一线ART治疗的儿童在4年期间具有良好的病毒学和耐药结果,无论CD4监测策略如何。许多检测到低水平病毒血症的儿童会自发重新抑制,这突出了在改用二线治疗前确认病毒学失败的重要性。VL反弹≥5000拷贝/毫升的儿童重新抑制的可能性要小得多,但NRTI耐药仅缓慢增加。这些结果与撒哈拉以南非洲地区越来越多接受一线ART治疗但病毒学监测可及性有限的HIV感染儿童相关。
ISRCTN注册库,ISRCTN编号:ISRCTN24791884 。