Facultad de Ciencias para la Salud, Universidad de Caldas, Manizales, Colombia.
Departmento de Fisioterapia, Universidad Federal de Rio Grande do Norte, Natal, Brasil.
Biomedica. 2021 Mar 19;41(1):111-122. doi: 10.7705/biomedica.5787.
Potentially inappropriate medication is associated with adverse health and functional outcomes, as well as increased health care costs.
To estimate the prevalence and types of potentially inappropriate medication according to the Beers criteria in community-dwelling older persons and to identify the major clinical and functional consequences of potentially inappropriate medication during two years of following.
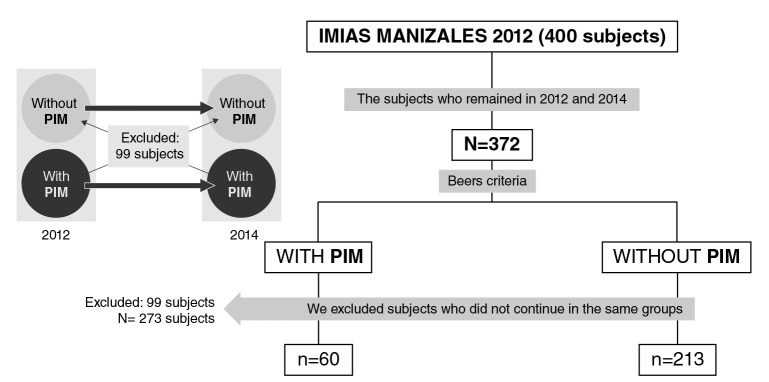
We conducted a longitudinal, descriptive, and observational study that included 400 65-year or older community-dwelling people (48% women) selected by simple random sampling in 2012. In 2014, 372 people were re-evaluated and classified into two groups based on the presence or absence of potentially inappropriate medication through the follow-up period.
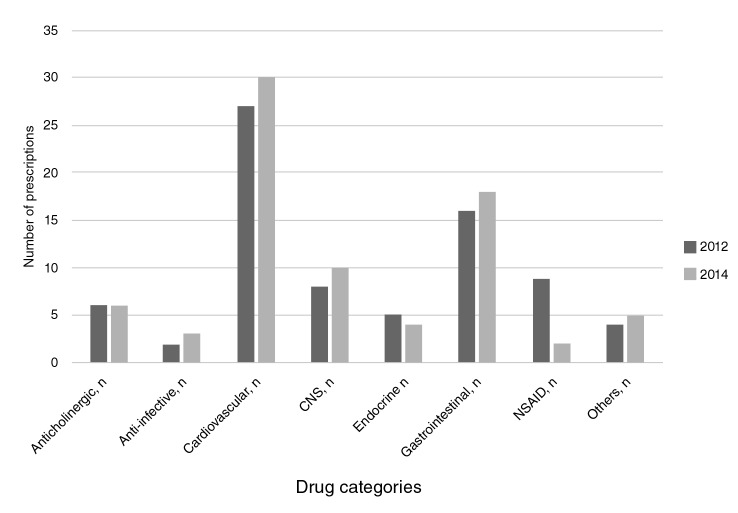
In total, 31% had polypharmacy (5-9 medications) and 1,8% had excessive polypharmacy (10 or more medications). The mean of the number of medications was higher in the potentially inappropriate medication group (3 vs. 5.78; p<0.001) and 21.9% still had the potentially inappropriate medication status during the follow-up; of them, 75% had one potentially inappropriate medication and 23% two. The presence of potentially inappropriate medication was more frequent among frail and depressed male individuals with a bad health self-assessment and comorbidities, especially diabetes mellitus and chronic obstructive pulmonary disease. In the group with sustained potentially inappropriate medication, we found a worsening health self-assessment, increased frailty, a higher incidence of recurrent falls and prevalence of depression, as well as a higher hospital admission rate, ambulatory medical consultation, and more prescribed medications. We did not find an impact on functional capacity.
We validated the negative effects of potentially inappropriate medication in the long run for the health of older people and, therefore, potentially inappropriate medications should be monitored in primary care services to avoid greater risks.
潜在不适当用药与不良健康和功能结果相关,同时也会增加医疗保健成本。
根据 Beers 标准评估社区居住的老年人中潜在不适当用药的发生率和类型,并确定在两年随访期间潜在不适当用药的主要临床和功能后果。
我们进行了一项纵向、描述性和观察性研究,纳入了 2012 年通过简单随机抽样选择的 400 名 65 岁及以上的社区居住者(48%为女性)。2014 年,对 372 名患者进行了重新评估,并根据随访期间潜在不适当用药的存在与否将其分为两组。
共有 31%的患者存在多种药物治疗(5-9 种药物),1.8%的患者存在过度多种药物治疗(10 种或更多药物)。潜在不适当用药组的平均用药数量更高(3 与 5.78;p<0.001),且在随访期间仍有 21.9%的患者存在潜在不适当用药状态;其中,75%的患者存在一种潜在不适当用药,23%的患者存在两种。潜在不适当用药在虚弱和抑郁的男性个体中更为常见,这些患者自我健康评估较差,合并症较多,尤其是糖尿病和慢性阻塞性肺疾病。在持续存在潜在不适当用药的患者中,我们发现健康自我评估恶化,虚弱程度加重,跌倒复发率和抑郁患病率增加,以及住院率、门诊医疗咨询和开处方药物数量增加。我们未发现对功能能力有影响。
我们验证了潜在不适当用药对老年人健康的长期负面影响,因此应在初级保健服务中监测潜在不适当用药,以避免更大的风险。