Division of Chronic Inflammation and Cancer, German Cancer Research Center (DKFZ), Heidelberg, Germany.
Liver Disease Research, Global Drug Discovery, Novo Nordisk A/S, Malov, Denmark.
Nature. 2021 Apr;592(7854):450-456. doi: 10.1038/s41586-021-03362-0. Epub 2021 Mar 24.
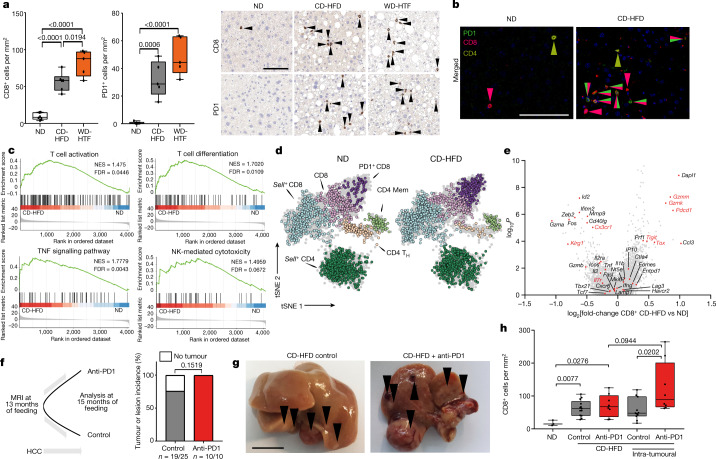
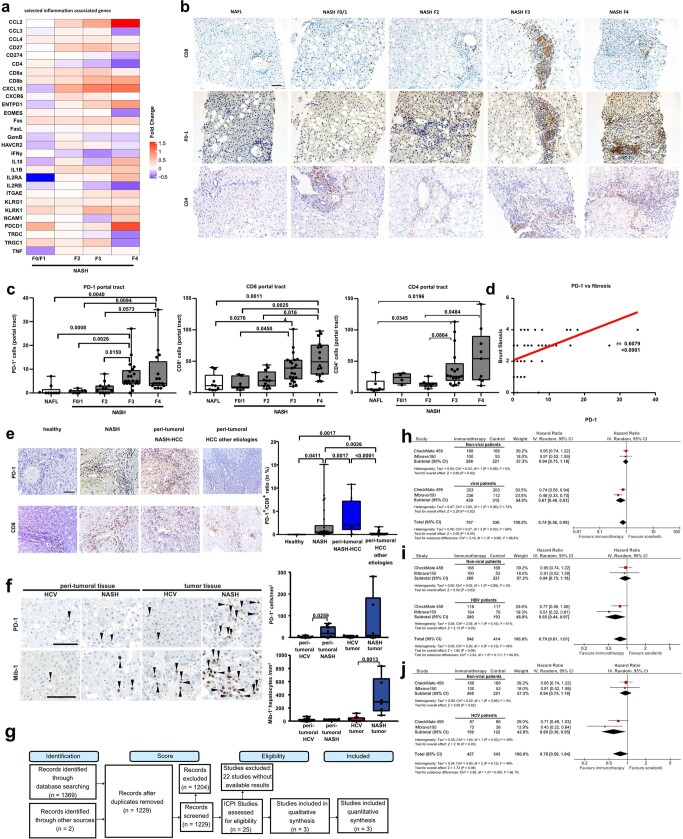
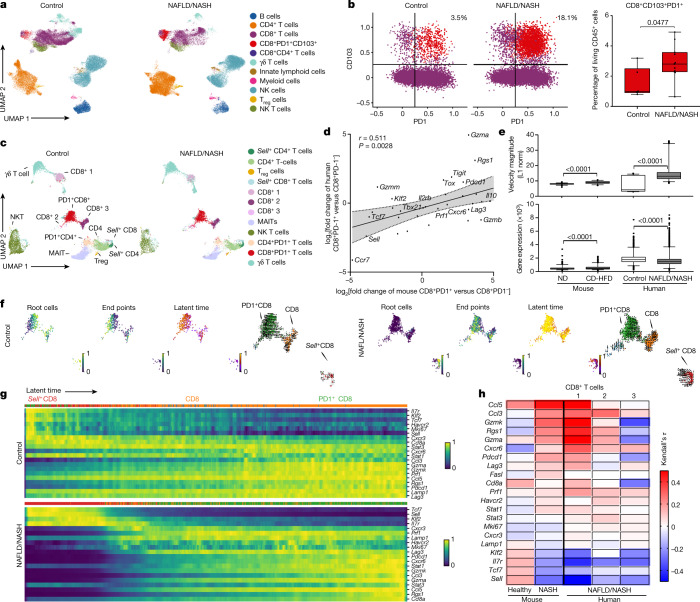
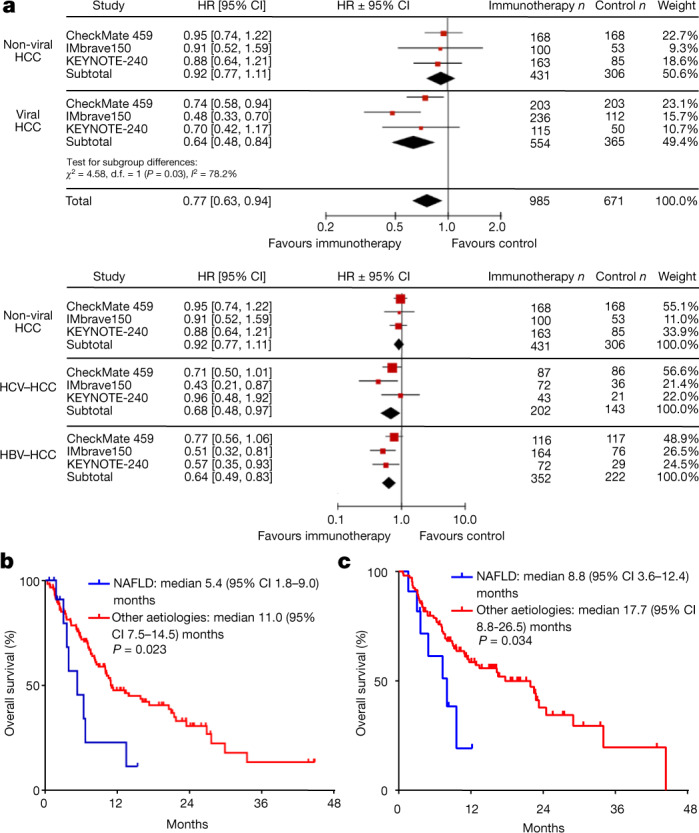
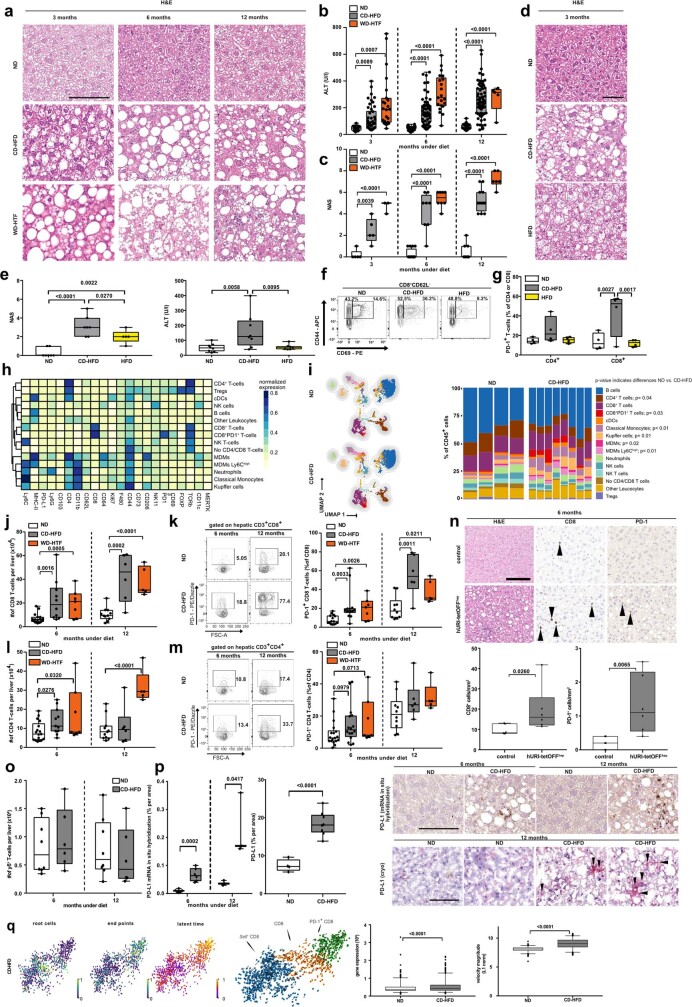
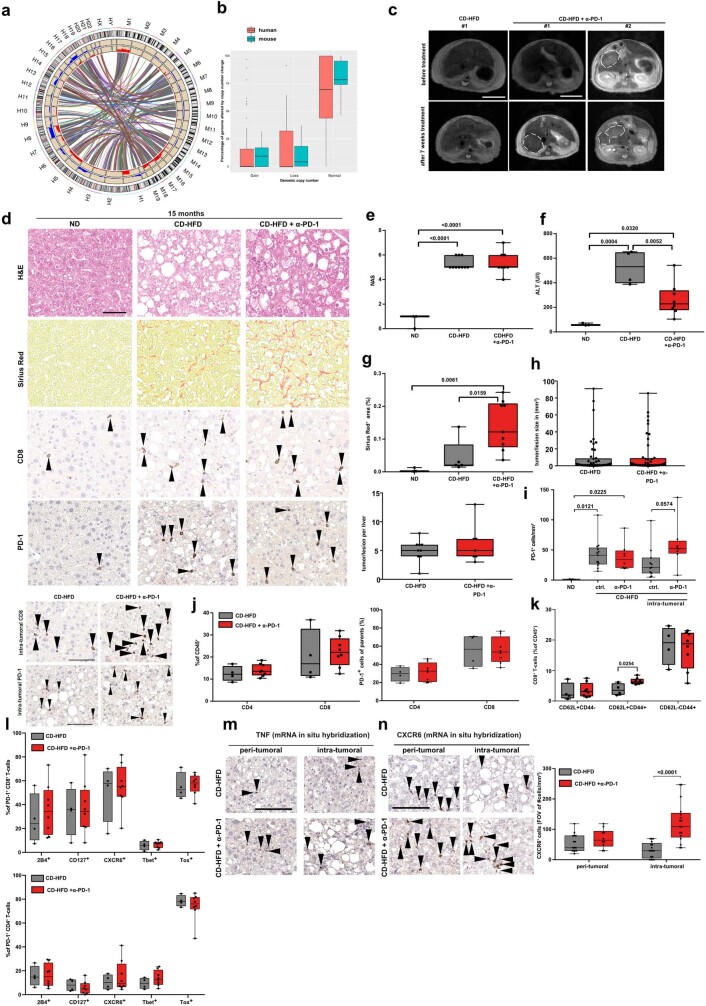
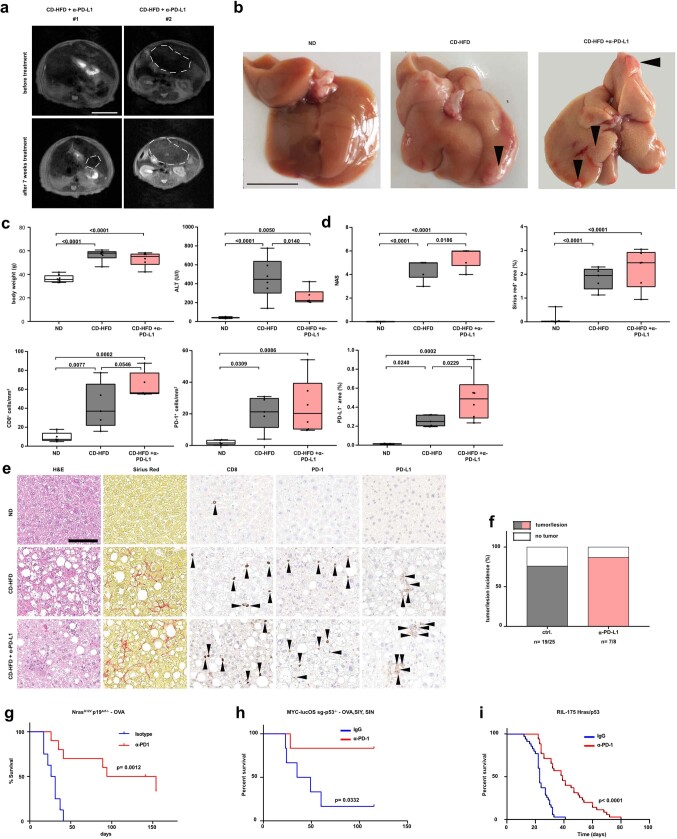
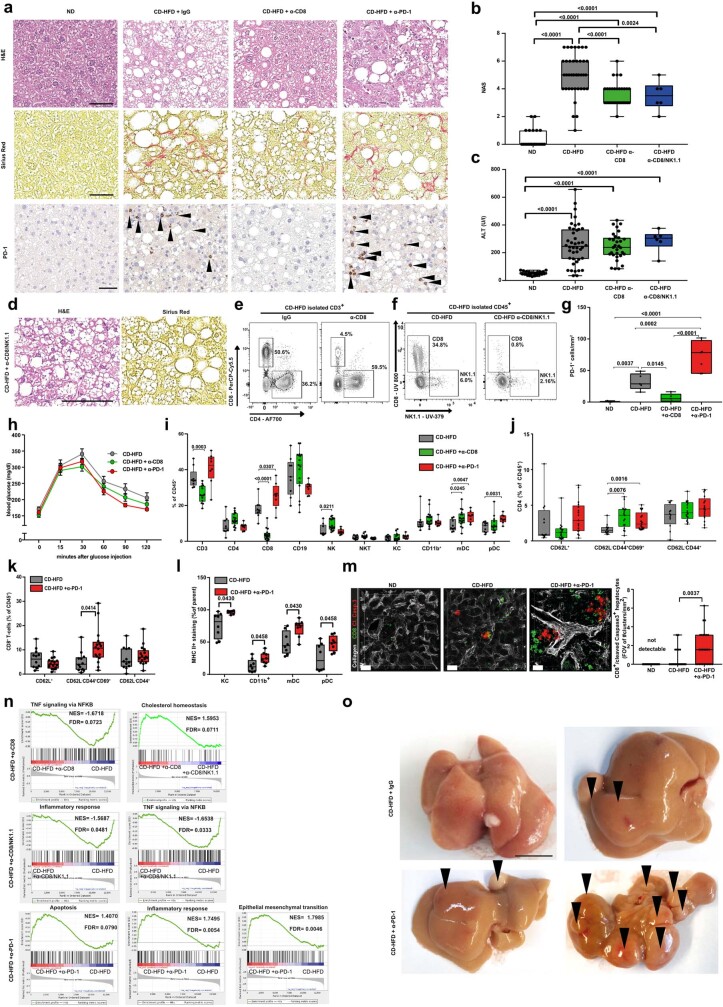
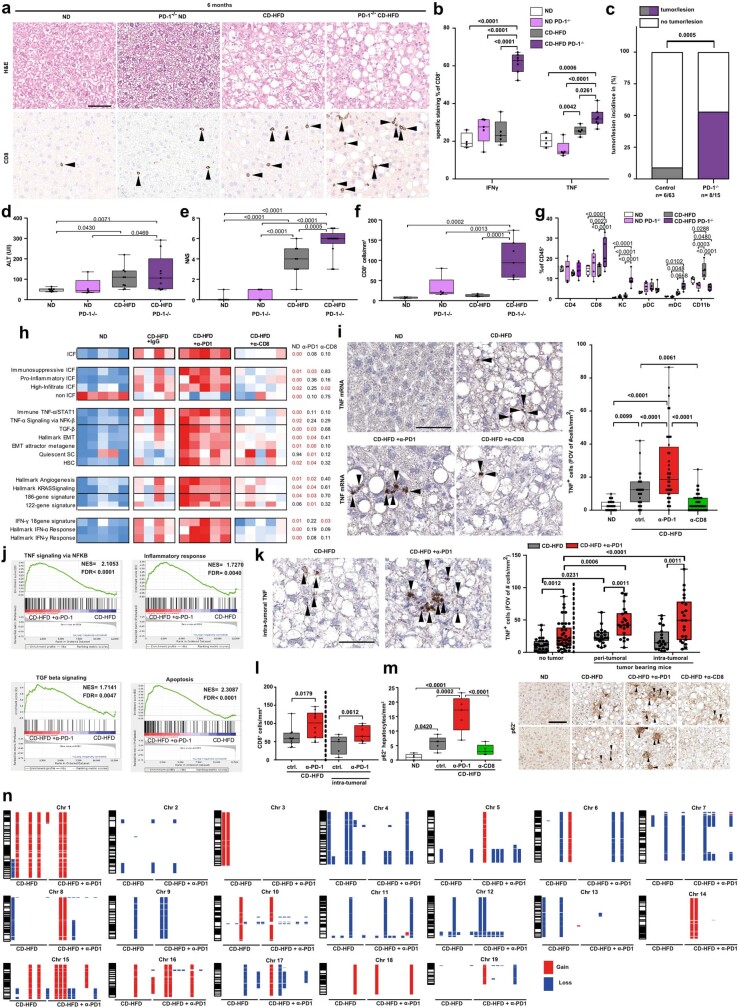
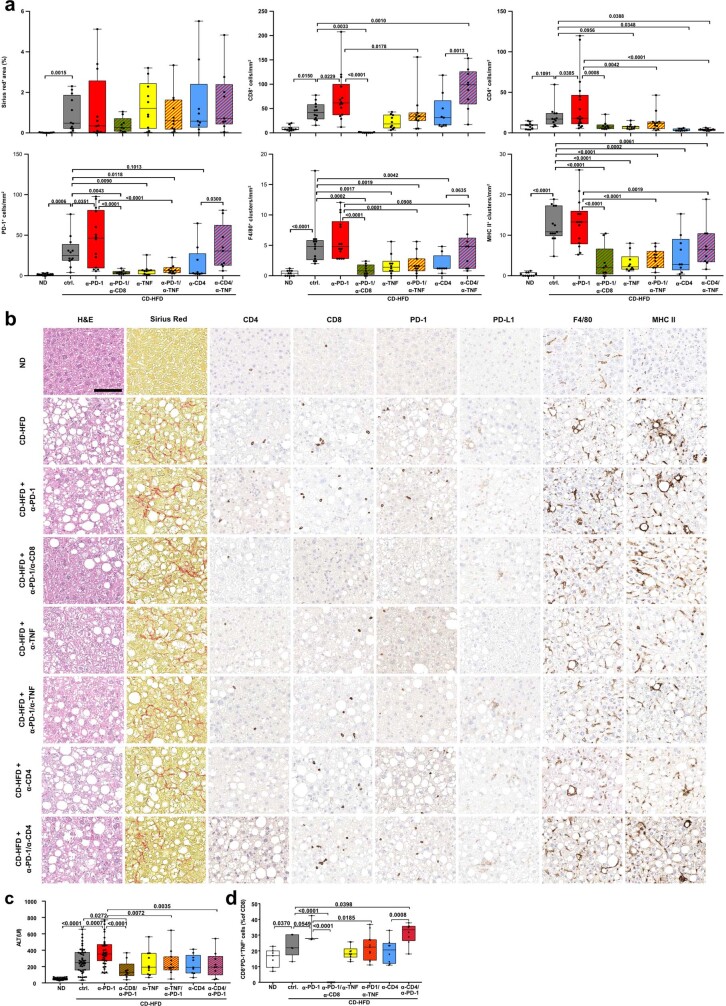
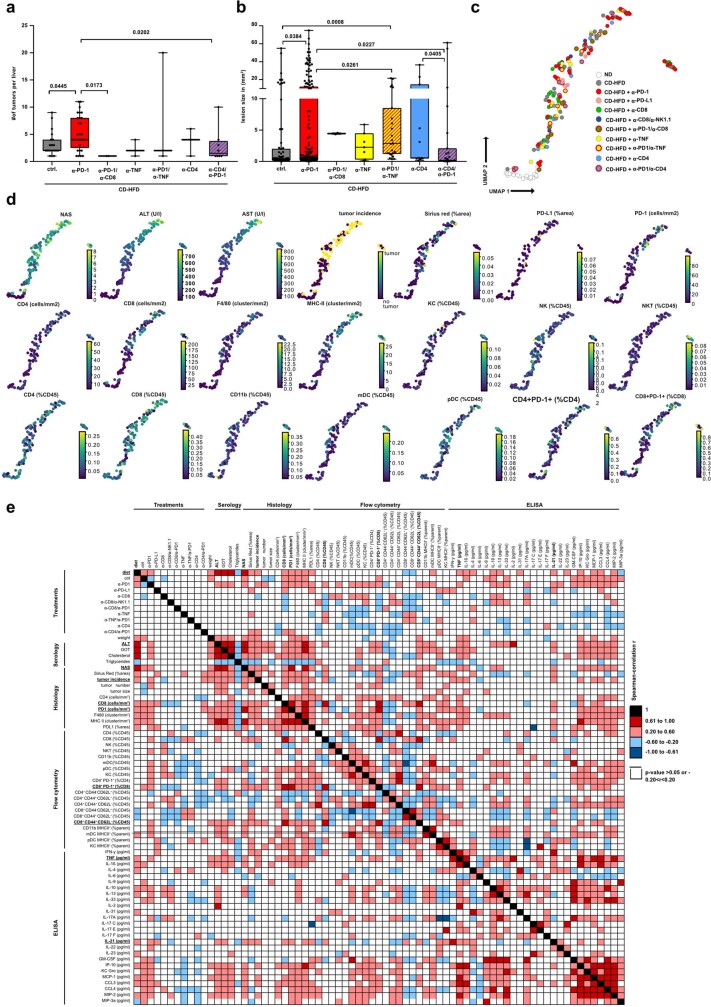
Hepatocellular carcinoma (HCC) can have viral or non-viral causes. Non-alcoholic steatohepatitis (NASH) is an important driver of HCC. Immunotherapy has been approved for treating HCC, but biomarker-based stratification of patients for optimal response to therapy is an unmet need. Here we report the progressive accumulation of exhausted, unconventionally activated CD8PD1 T cells in NASH-affected livers. In preclinical models of NASH-induced HCC, therapeutic immunotherapy targeted at programmed death-1 (PD1) expanded activated CD8PD1 T cells within tumours but did not lead to tumour regression, which indicates that tumour immune surveillance was impaired. When given prophylactically, anti-PD1 treatment led to an increase in the incidence of NASH-HCC and in the number and size of tumour nodules, which correlated with increased hepatic CD8PD1CXCR6, TOX, and TNF T cells. The increase in HCC triggered by anti-PD1 treatment was prevented by depletion of CD8 T cells or TNF neutralization, suggesting that CD8 T cells help to induce NASH-HCC, rather than invigorating or executing immune surveillance. We found similar phenotypic and functional profiles in hepatic CD8PD1 T cells from humans with NAFLD or NASH. A meta-analysis of three randomized phase III clinical trials that tested inhibitors of PDL1 (programmed death-ligand 1) or PD1 in more than 1,600 patients with advanced HCC revealed that immune therapy did not improve survival in patients with non-viral HCC. In two additional cohorts, patients with NASH-driven HCC who received anti-PD1 or anti-PDL1 treatment showed reduced overall survival compared to patients with other aetiologies. Collectively, these data show that non-viral HCC, and particularly NASH-HCC, might be less responsive to immunotherapy, probably owing to NASH-related aberrant T cell activation causing tissue damage that leads to impaired immune surveillance. Our data provide a rationale for stratification of patients with HCC according to underlying aetiology in studies of immunotherapy as a primary or adjuvant treatment.
肝细胞癌(HCC)可由病毒或非病毒因素引起。非酒精性脂肪性肝炎(NASH)是 HCC 的重要驱动因素。免疫疗法已被批准用于治疗 HCC,但基于生物标志物对患者进行分层以实现最佳治疗反应是未满足的需求。在这里,我们报告了在 NASH 影响的肝脏中耗尽的、非常规激活的 CD8PD1 T 细胞的逐渐积累。在 NASH 诱导的 HCC 的临床前模型中,针对程序性死亡受体 1(PD1)的治疗性免疫疗法在肿瘤内扩增了激活的 CD8PD1 T 细胞,但并未导致肿瘤消退,这表明肿瘤免疫监视受损。预防性给予抗 PD1 治疗会导致 NASH-HCC 的发生率增加,肿瘤结节的数量和大小增加,这与肝内 CD8PD1CXCR6、TOX 和 TNF T 细胞的增加相关。抗 PD1 治疗引发的 HCC 增加可通过耗尽 CD8 T 细胞或 TNF 中和来预防,这表明 CD8 T 细胞有助于诱导 NASH-HCC,而不是增强或执行免疫监视。我们在患有 NAFLD 或 NASH 的人类肝脏中的 CD8PD1 T 细胞中发现了类似的表型和功能特征。对超过 1600 名晚期 HCC 患者进行的三种 PD-L1(程序性死亡配体 1)或 PD1 抑制剂的随机 III 期临床试验的荟萃分析表明,免疫疗法并未改善非病毒性 HCC 患者的生存率。在另外两个队列中,接受抗 PD1 或抗 PD-L1 治疗的 NASH 驱动 HCC 患者的总生存期较其他病因患者缩短。总的来说,这些数据表明非病毒性 HCC,特别是 NASH-HCC,可能对免疫疗法的反应较差,可能是由于 NASH 相关的异常 T 细胞激活导致组织损伤,从而导致免疫监视受损。我们的数据为根据 HCC 患者的潜在病因对接受免疫治疗作为一线或辅助治疗的 HCC 患者进行分层提供了依据。