NAFLD Research Center, Division of Gastroenterology and Hepatology, Department of Medicine, University of California at San Diego, La Jolla, CA, USA.
Department of Internal Medicine, College of Medicine, Yeungnam University, Daegu, South Korea.
Aliment Pharmacol Ther. 2021 May;53(9):1030-1037. doi: 10.1111/apt.16324. Epub 2021 Mar 25.
Magnetic resonance elastography (MRE) is a reliable non-invasive alternative to liver biopsy for assessing liver fibrosis. There are limited data regarding an association between liver fibrosis by MRE and risk of cardiovascular disease (CVD).
To investigate the association of high-risk CVD phenotype determined by coronary artery calcification (CAC) with liver fibrosis by MRE in patients with non-alcoholic fatty liver disease (NAFLD).
This was a cross-sectional analysis of well-characterised, prospective cohorts including 105 patients with NAFLD (MR imaging-derived proton density fat fraction ≥ 5%) with contemporaneous cardiac computed tomography (CT) and MRE. Patients were assessed using MRE for liver stiffness, and cardiac CT for the presence of CAC (defined as coronary artery calcium score > 0). Odds of presence of CAC were analysed using logistic regression analysis.
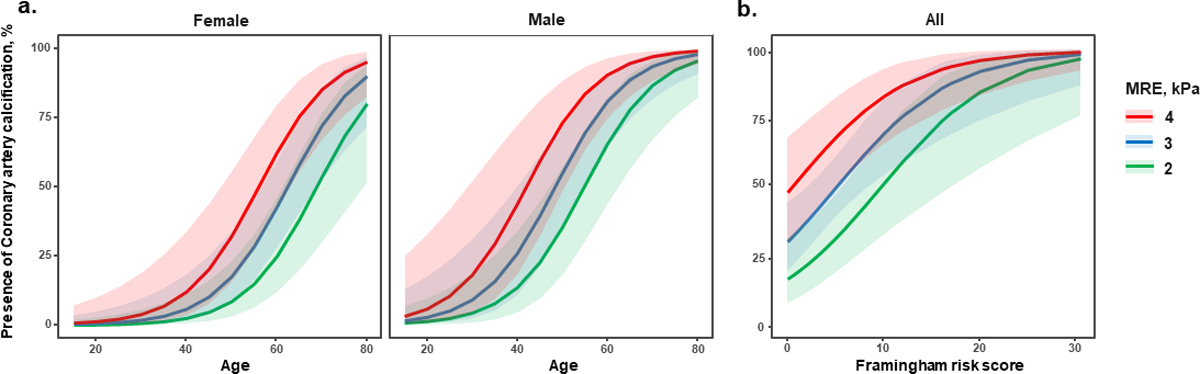
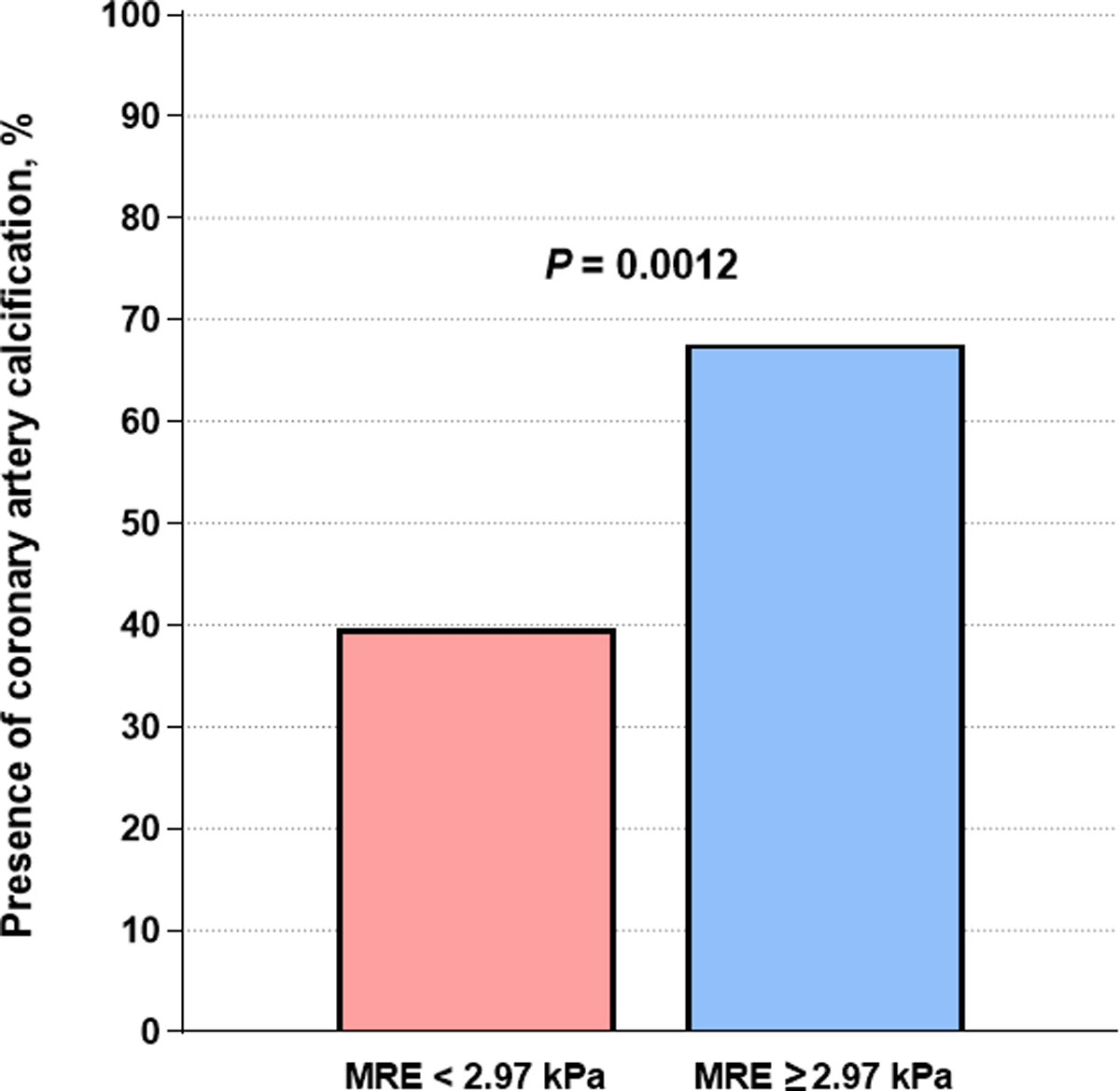
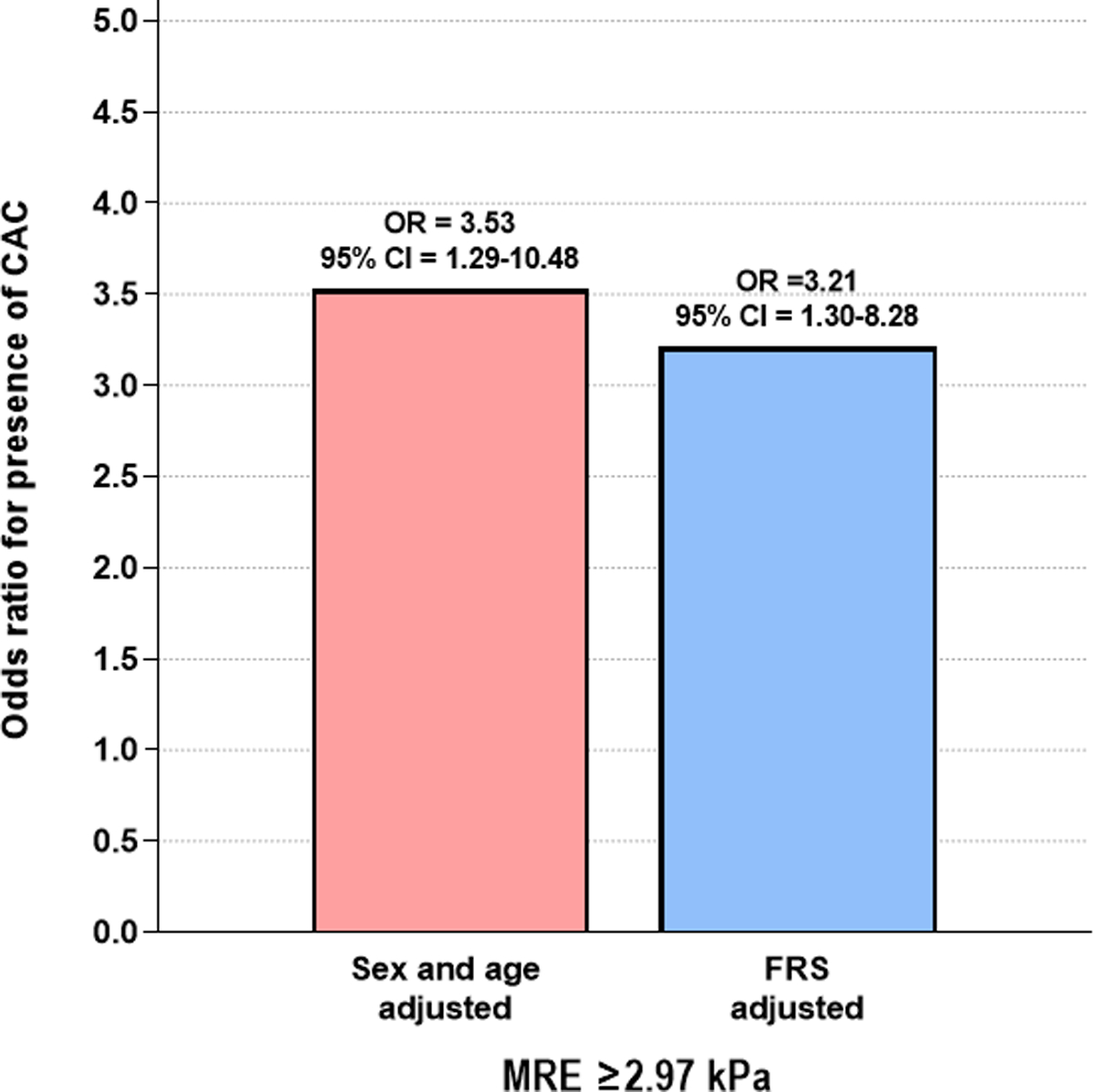
The average age and body mass index were 54.9 years and 32.9 kg/m respectively. In this cohort, 49.5% of patients had CAC and 35.2% had significant liver fibrosis (defined as MRE ≥2.97 kPa). Compared to patients without CAC, those with CAC were older (50.0 [39.0-59.0] vs 63.0 [55.5-67.5], P < 0.001) and had higher Framingham risk score (FRS, 1.0 [0.5-3.5] vs 6.0 [2.0-12.0], P < 0.001). In multivariable-adjusted analysis, liver stiffness as a continuous trait on MRE was independently associated with the presence of CAC in a sex and age-adjusted model (adjusted odd ratios [aOR] = 2.23, 95% confidence interval [CI] = 1.31-4.34, P = 0.007) as well as in a FRS-adjusted model (aOR = 2.16, 95% CI = 1.29-4.09, P = 0.008). When analysed as a dichotomous trait, significant fibrosis (MRE-stiffness ≥2.97 kPa) remained independently associated with the presence of CAC in both FRS-adjusted model and sex and age-adjusted model (aOR = 3.21-3.53, P = 0.013-0.017). In addition, CAC was more prevalent in patients with significant fibrosis than those without as determined by MRE (67.6% vs 39.7%, P = 0.012).
Liver stiffness determined by MRE is an independent predictor for the presence of CAC in patients with NAFLD. Patients with NAFLD and significant fibrosis by MRE should be considered for further cardiovascular risk assessment, regardless of their FRS.
磁共振弹性成像(MRE)是一种可靠的非侵入性替代肝活检的方法,可用于评估肝纤维化。关于 MRE 评估的肝纤维化与心血管疾病(CVD)风险之间的关联,数据有限。
探讨非酒精性脂肪性肝病(NAFLD)患者中,由冠状动脉钙化(CAC)确定的高风险 CVD 表型与 MRE 评估的肝纤维化之间的关系。
这是一项对特征明确的前瞻性队列的横断面分析,包括 105 例 NAFLD 患者(MR 成像衍生质子密度脂肪分数≥5%),同时进行心脏计算机断层扫描(CT)和 MRE。使用 MRE 评估肝硬度,使用心脏 CT 评估 CAC 的存在(定义为冠状动脉钙评分>0)。使用逻辑回归分析评估 CAC 存在的可能性。
平均年龄和体重指数分别为 54.9 岁和 32.9kg/m2。在该队列中,49.5%的患者有 CAC,35.2%的患者有明显的肝纤维化(定义为 MRE≥2.97kPa)。与无 CAC 的患者相比,有 CAC 的患者年龄更大(50.0[39.0-59.0] vs 63.0[55.5-67.5],P<0.001)且Framingham 风险评分更高(FRS,1.0[0.5-3.5] vs 6.0[2.0-12.0],P<0.001)。在多变量调整分析中,MRE 上肝硬度作为连续特征,在性别和年龄调整模型中与 CAC 的存在独立相关(调整后的比值比[aOR]2.23,95%置信区间[CI]1.31-4.34,P=0.007),在 FRS 调整模型中也与 CAC 的存在独立相关(aOR 2.16,95%CI 1.29-4.09,P=0.008)。当作为二分类特征进行分析时,MRE 确定的显著纤维化(MRE 硬度≥2.97kPa)在 FRS 调整模型和性别及年龄调整模型中与 CAC 的存在均独立相关(aOR 3.21-3.53,P=0.013-0.017)。此外,与 MRE 确定无显著纤维化的患者相比,有显著纤维化的患者 CAC 的患病率更高(67.6% vs 39.7%,P=0.012)。
MRE 确定的肝硬度是 NAFLD 患者 CAC 存在的独立预测因子。无论 FRS 如何,MRE 确定有显著纤维化的 NAFLD 患者均应考虑进一步进行心血管风险评估。