School of Public Health, Faculty of Medicine, The University of Queensland, Brisbane, Queensland, Australia.
Public Health Unit, Central Queensland Hospital and Health Service, Rockhampton, Queensland, Australia.
BMJ Open. 2021 Mar 26;11(3):e044649. doi: 10.1136/bmjopen-2020-044649.
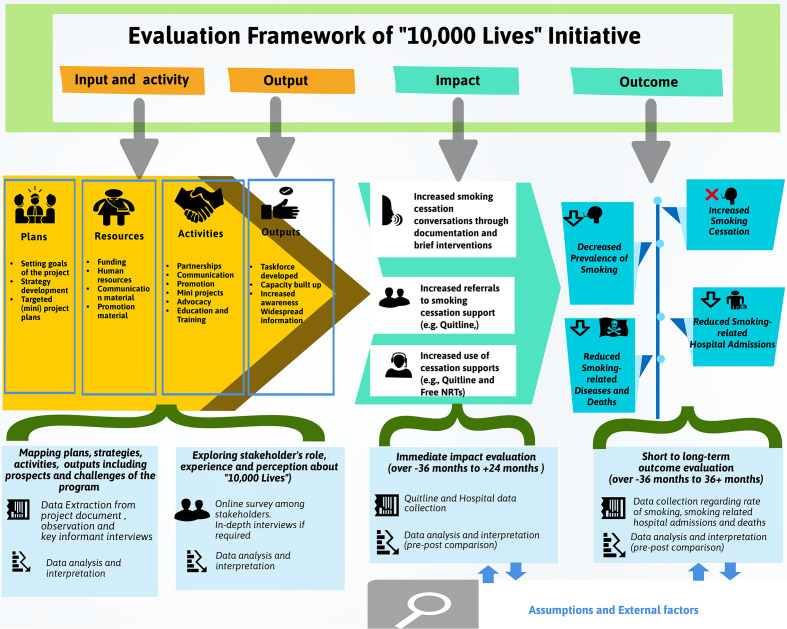
This study used a programme logic model to describe the inputs, activities and outputs of the '10,000 Lives' smoking cessation initiative in Central Queensland, Australia.
A programme logic model provided the framework for the process evaluation of '10,000 Lives'. The data were collected through document review, observation and key informant interviews and subsequently analysed after coding and recoding into classified themes, inputs, activities and outputs.
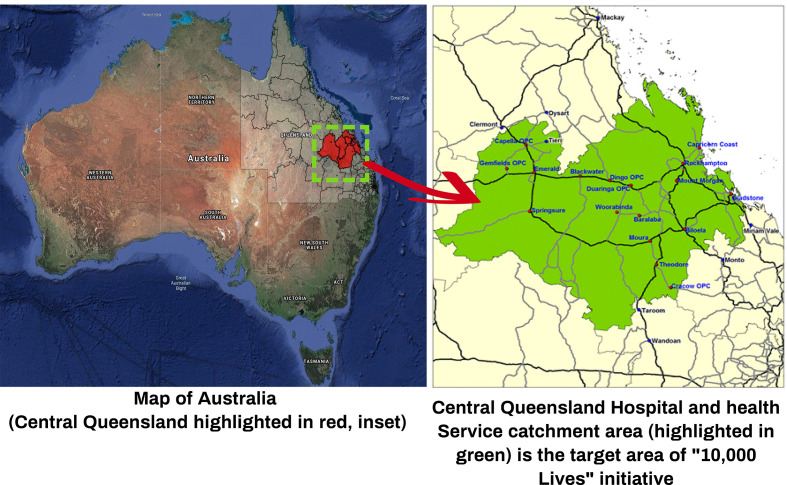
The prevalence of smoking is higher in the Central Queensland region of Australia compared with the national and state averages. In 2017, Central Queensland Hospital and Health Services set a target to reduce the percentage of adults who smoke from 16.7% to 9.5% in the Central Queensland region by 2030 as part of their strategic vision ('Destination 2030'). Achieving this target is equivalent to 20,000 fewer smokers in Central Queensland, which should result in 10,000 fewer premature deaths due to smoking-related diseases. To translate this strategic goal into an actionable smoking cessation initiative, the '10,000 Lives' health promotion programme was officially launched on 1 November 2017.
The activities of the initiative coordinated by a senior project officer included building clinical and community taskforces, organising summits and workshops, and regular communications to stakeholders. Public communication strategies (e.g., Facebook, radio, community exhibitions of '10,000 Lives' and health-related events) were used to promote available smoking cessation support to the Central Queensland community.
The '10,000 Lives' initiative provides an example of a coordinated health promotion programme to increase smoking cessation in a regional area through harnessing existing resources and strategic partnerships (e.g., Quitline). Documenting and describing the process evaluation of the '10,000 Lives' model is important so that it can be replicated in other regional areas with high prevalence of smoking.
本研究采用计划逻辑模型描述澳大利亚昆士兰州中部“万人生存”戒烟计划的投入、活动和产出。
计划逻辑模型为“万人生存”的过程评估提供了框架。数据通过文件审查、观察和关键知情人访谈收集,随后进行编码和重新编码为分类主题、投入、活动和产出进行分析。
与全国和州平均水平相比,澳大利亚昆士兰州中部地区的吸烟率较高。2017 年,昆士兰州中部地区医院和卫生服务机构将目标设定为,到 2030 年,将该地区成年人吸烟率从 16.7%降至 9.5%,作为其战略愿景(“2030 年目标”)的一部分。实现这一目标相当于在昆士兰州中部减少 2 万名吸烟者,这将导致与吸烟相关的疾病导致的 1 万人过早死亡。为了将这一战略目标转化为可行的戒烟计划,“万人生存”健康促进计划于 2017 年 11 月 1 日正式启动。
由一名高级项目官员协调的计划活动包括建立临床和社区工作队、组织峰会和研讨会,以及与利益攸关方定期沟通。公共沟通策略(如 Facebook、广播、“万人生存”社区展览和与健康相关的活动)用于向昆士兰州中部社区宣传可用的戒烟支持。
“万人生存”计划为通过利用现有资源和战略伙伴关系(如戒烟热线)在区域范围内提高戒烟率的协调健康促进计划提供了一个范例。记录和描述“万人生存”模型的过程评估非常重要,以便在其他吸烟率较高的地区进行复制。