Mohamed Mohamed Bakr, Ali Mohamed Hassan, Shamaa Mostafa A, Shaaban Sami M
Department of Urology, Faculty of Medicine, Port Said University, Port Said, Egypt.
Department of Urology, Faculty of Medicine, Suez Canal University, Ismailia, Egypt.
Urol Ann. 2020 Oct-Dec;12(4):360-365. doi: 10.4103/UA.UA_137_19. Epub 2020 Oct 15.
The objective of the study was to compare maintenance versus single course of intravesical Bacillus Calmette-Guerin (BCG) in the management of high-risk nonmuscle invasive bladder cancer (NMIBC) regarding recurrence, progression, survival, and complications.
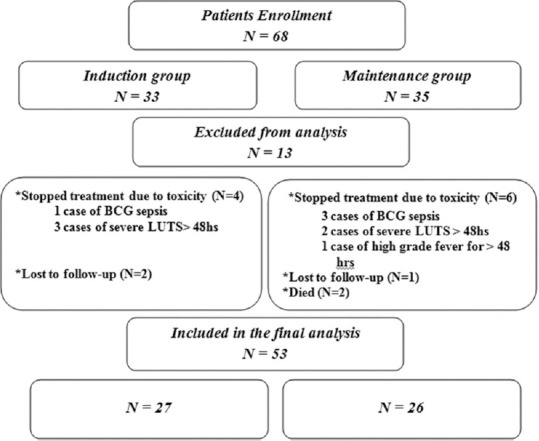
After transurethral resection of bladder tumor (TURBT), Group I patients (33) received weekly doses of 90 mg of live attenuated Pasteur strain of BCG. The course was started 14 days after the second TURBT for 6 consecutive weeks. In Group II: 35 patients, the induction schedule was followed by 3 weekly instillations at months 3, 6, and 12 as a maintenance course. Recurrence, progression rates, survival, and toxicity were assessed in both the groups.
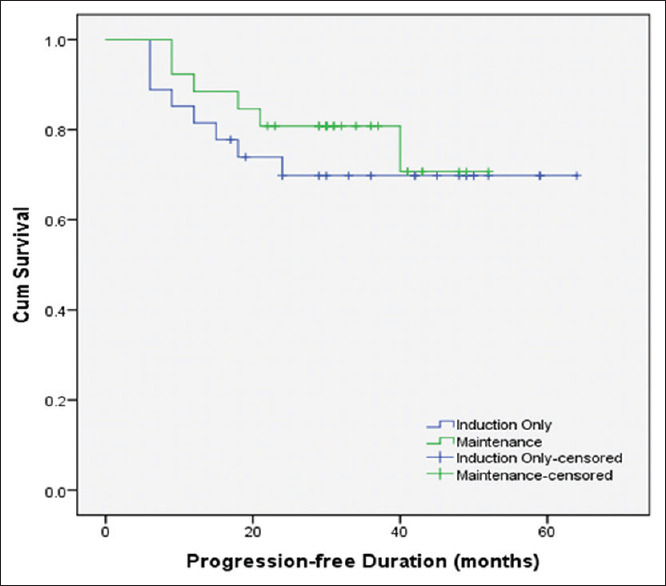
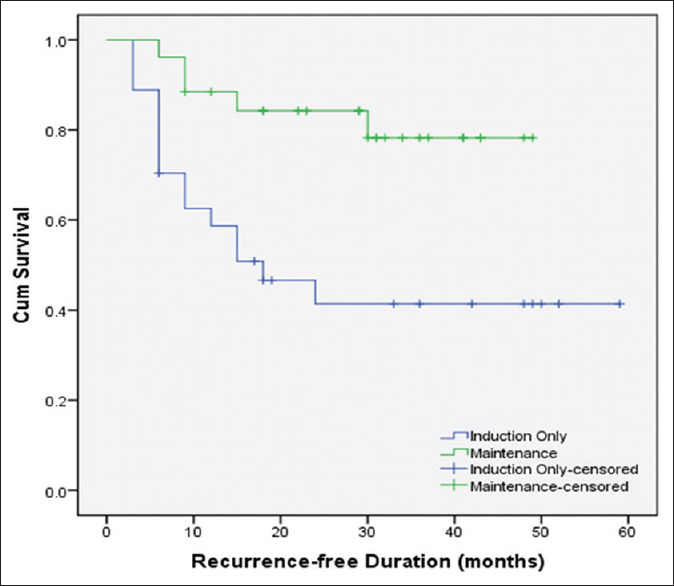
Patients with induction therapy alone had significantly higher recurrence rate than those received maintenance therapy (55.6% vs. 19.2%, = 0.01). The 5-year recurrence-free survival rate was 41% and 78% in both the groups, respectively. There was no significant difference regarding the progression rate for both the groups. The mean 5-year progression-free time was comparable between the two groups. The 5-year progression-free survival was 69.8% for patients who underwent induction therapy alone compared to 70.7% for maintenance therapy. Overall local adverse events were significantly higher in patients who underwent maintenance treatment protocol.
SPSS package version 20 and Kaplan-Meier curves were used to evaluate the survival rate.
Maintenance doses of BCG significantly decrease and delay the recurrence of high-risk NMIBC. However, there is no significant favor as regards tumor progression. Maintenance doses of BCG are significantly associated with a higher incidence of local adverse effects than induction doses alone.
本研究的目的是比较维持性膀胱内灌注卡介苗(BCG)与单次膀胱内灌注BCG在高危非肌层浸润性膀胱癌(NMIBC)的复发、进展、生存及并发症管理方面的差异。
膀胱肿瘤经尿道切除术(TURBT)后,第一组患者(33例)接受每周90mg减毒活卡介苗巴斯德菌株的剂量。疗程在第二次TURBT后14天开始,连续6周。第二组:35例患者,诱导方案后在第3、6和12个月进行3次每周一次的灌注作为维持疗程。对两组患者的复发率、进展率、生存率和毒性进行评估。
单纯接受诱导治疗的患者复发率显著高于接受维持治疗的患者(55.6%对19.2%,P = 0.01)。两组的5年无复发生存率分别为41%和78%。两组的进展率无显著差异。两组的平均5年无进展时间相当。单纯接受诱导治疗的患者5年无进展生存率为69.8%,而维持治疗为70.7%。接受维持治疗方案的患者总体局部不良事件显著更高。
采用SPSS 20版软件包和Kaplan-Meier曲线评估生存率。
BCG维持剂量可显著降低并延迟高危NMIBC的复发。然而,在肿瘤进展方面无显著优势。与单独诱导剂量相比,BCG维持剂量与局部不良反应的更高发生率显著相关。