Meneghini Maria, Crespo Elena, Niemann Matthias, Torija Alba, Lloberas Nuria, Pernin Vincent, Fontova Pere, Melilli Edoardo, Favà Alexandre, Montero Nuria, Manonelles Anna, Cruzado Josep Maria, Palou Eduard, Martorell Jaume, Grinyó Josep Maria, Bestard Oriol
Kidney Transplant Unit, Nephrology Department, Bellvitge University Hospital, Barcelona, Spain.
Translational Transplantation and Nephrology Laboratory, Institut d'Investigació Biomèdica de Bellvitge (IDIBELL), Barcelona, Spain.
Front Immunol. 2021 Mar 10;11:623276. doi: 10.3389/fimmu.2020.623276. eCollection 2020.
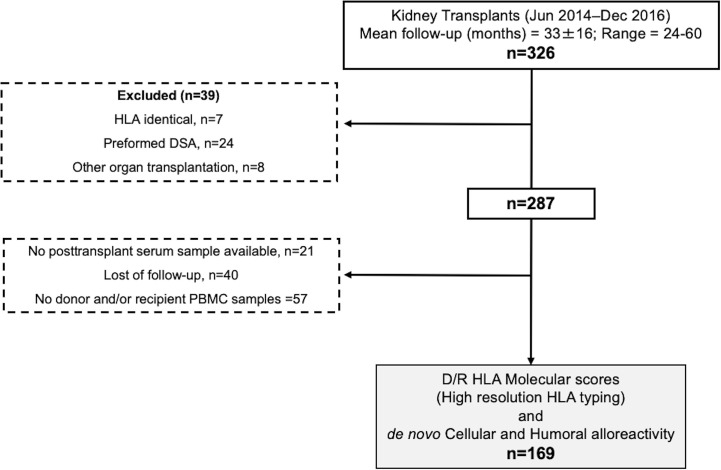
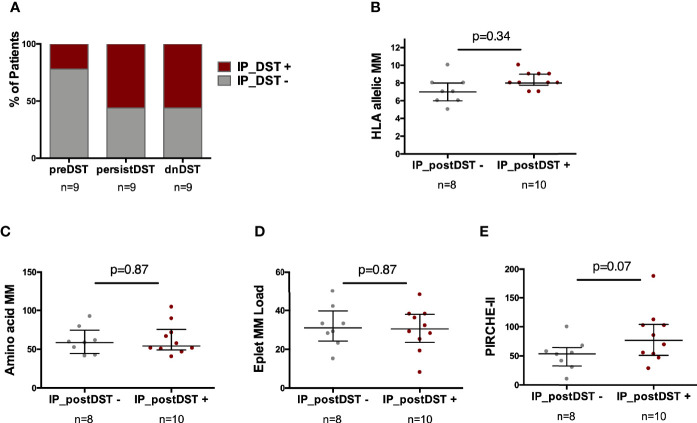
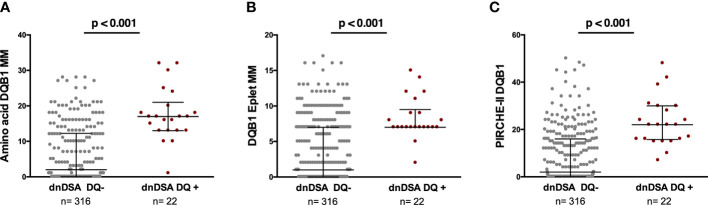
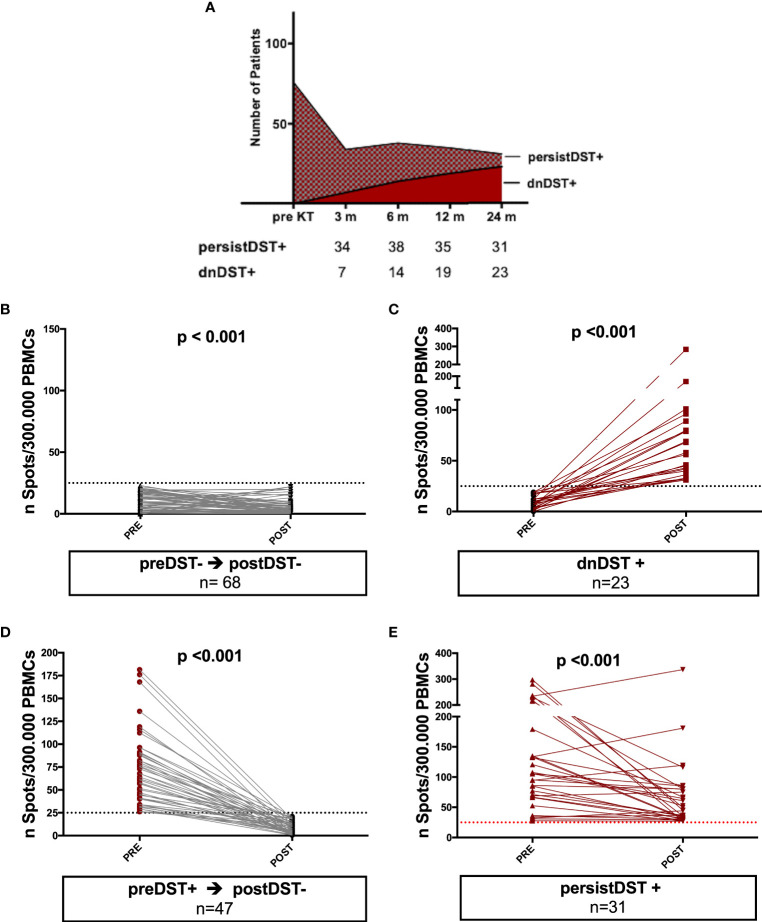
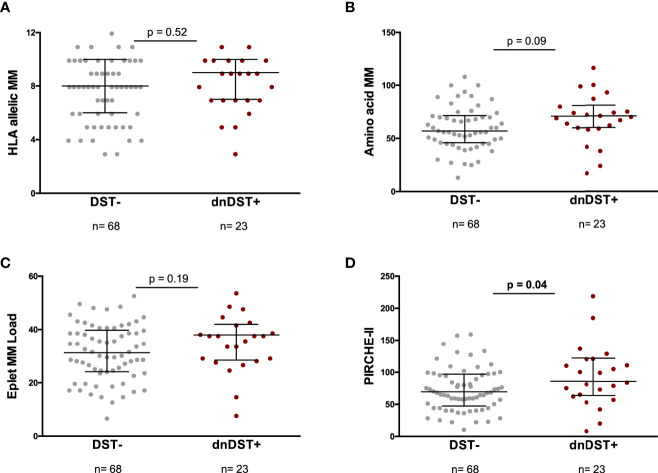
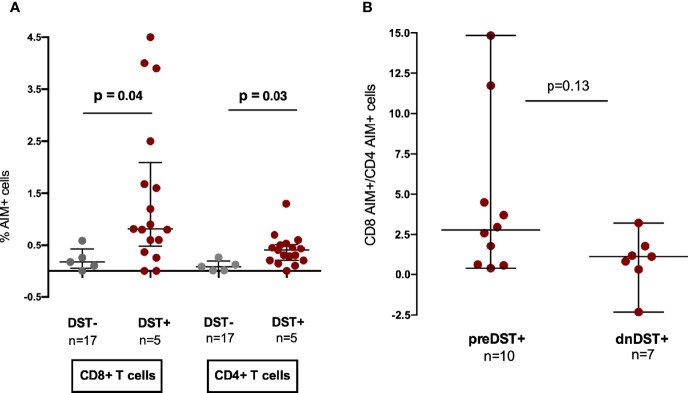
Donor/recipient molecular human leukocyte antigen (HLA) mismatch predicts primary B-cell alloimmune activation, yet the impact on donor-specific T-cell alloimmunity (dnDST) remains undetermined. The hypothesis of our study is that donor/recipient HLA mismatches assessed at the molecular level may also influence a higher susceptibility to the development of posttransplant primary T-cell alloimmunity. In this prospective observational study, 169 consecutive kidney transplant recipients without preformed donor-specific antibodies (DSA) and with high resolution donor/recipient HLA typing were evaluated for HLA molecular mismatch scores using different informatic algorithms [amino acid mismatch, eplet MM, and Predicted Indirectly Recognizable HLA Epitopes (PIRCHE-II)]. Primary donor-specific alloimmune activation over the first 2 years posttransplantation was assessed by means of both dnDSA and dnDST using single antigen bead (SAB) and IFN-γ ELISPOT assays, respectively. Also, the predominant alloantigen presenting pathway priming DST alloimmunity and the contribution of main alloreactive T-cell subsets were further characterized . Pretransplantation, 78/169 (46%) were DST+ whereas 91/169 (54%) DST-. At 2 years, 54/169 (32%) patients showed detectable DST responses: 23/54 (42%) dnDST and 31/54 (57%) persistently positive (persistDST+). 24/169 (14%) patients developed dnDSA. A strong correlation was observed between the three distinct molecular mismatch scores and they all accurately predicted dnDSA formation, in particular at the DQ locus. Likewise, HLA molecular incompatibility predicted the advent of dnDST, especially when assessed by PIRCHE-II score (OR 1.014 95% CI 1.001-1.03, p=0.04). While pretransplant DST predicted the development of posttransplant BPAR (OR 5.18, 95% CI=1.64-16.34, p=0.005) and particularly T cell mediated rejection (OR 5.33, 95% CI=1.45-19.66, p=0.012), patients developing dnDST were at significantly higher risk of subsequent dnDSA formation (HR 2.64, 95% CI=1.08-6.45, p=0.03). experiments showed that unlike preformed DST that is predominantly primed by CD8+ direct pathway T cells, posttransplant DST may also be activated by the indirect pathway of alloantigen presentation, and predominantly driven by CD4+ alloreactive T cells in an important proportion of patients. donor-specific cellular alloreactivity seems to precede subsequent humoral alloimmune activation and is influenced by a poor donor/recipient HLA molecular matching.
供体/受体分子人类白细胞抗原(HLA)错配可预测原发性B细胞同种免疫激活,但对供体特异性T细胞同种免疫(dnDST)的影响仍未确定。我们研究的假设是,在分子水平评估的供体/受体HLA错配也可能影响移植后原发性T细胞同种免疫发展的更高易感性。在这项前瞻性观察研究中,对169例连续的肾移植受者进行了评估,这些受者没有预先形成的供体特异性抗体(DSA),并且进行了高分辨率的供体/受体HLA分型,使用不同的信息学算法[氨基酸错配、表位错配(eplet MM)和预测的间接可识别HLA表位(PIRCHE-II)]计算HLA分子错配分数。在移植后的前2年,分别使用单抗原珠(SAB)和IFN-γ ELISPOT试验通过dnDSA和dnDST评估原发性供体特异性同种免疫激活。此外,进一步明确了引发DST同种免疫的主要同种抗原呈递途径以及主要同种反应性T细胞亚群的贡献。移植前,78/169(46%)为DST阳性,而91/169(54%)为DST阴性。在2年时,54/169(32%)的患者出现了可检测到的DST反应:23/54(42%)为dnDST,31/54(57%)持续阳性(persistDST+)。24/169(14%)的患者产生了dnDSA。观察到三种不同的分子错配分数之间存在强相关性,并且它们都准确地预测了dnDSA的形成,特别是在DQ位点。同样,HLA分子不相容性预测了dnDST的出现,尤其是通过PIRCHE-II评分评估时(OR 1.014,95%CI 1.001-1.03,p=0.04)。虽然移植前的DST预测了移植后BPAR的发生(OR 5.18,95%CI=1.64-16.34,p=0.005),特别是T细胞介导的排斥反应(OR 5.33,95%CI=1.45-19.66,p=0.012),但发生dnDST的患者随后形成dnDSA的风险显著更高(HR 2.64,95%CI=1.08-6.45,p=0.03)。实验表明,与主要由CD8+直接途径T细胞引发的预先形成的DST不同,移植后的DST也可能通过同种抗原呈递的间接途径被激活,并且在相当一部分患者中主要由CD4+同种反应性T细胞驱动。供体特异性细胞同种反应性似乎先于随后的体液同种免疫激活,并且受到供体/受体HLA分子匹配不佳的影响。