Wang Zhixian, Wang Jing, Zhu Yunpeng, Liu Chang, Li Xing, Zeng Xiaoyong
Department of Urology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Department of General Medical, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Front Oncol. 2021 Mar 10;11:604724. doi: 10.3389/fonc.2021.604724. eCollection 2021.
More T1N0M0 renal cell carcinoma (RCC) is detected and the prognosis has improved, but, the current focus on non-RCC-related mortality is superficial. We investigated cause-specific mortality and its temporal patterns after an RCC diagnosis.
In the Surveillance, Epidemiology, and End Results-18 database, patients with T1N0M0 RCC treated with partial nephrectomy (PN) or radical nephrectomy (RN) during 2000-15 were identified. Standardized mortality ratios (SMRs) for cause of death were calculated. Risk predictors for each cause-specific mortality were investigated using the Fine and Gray sub-distribution model.
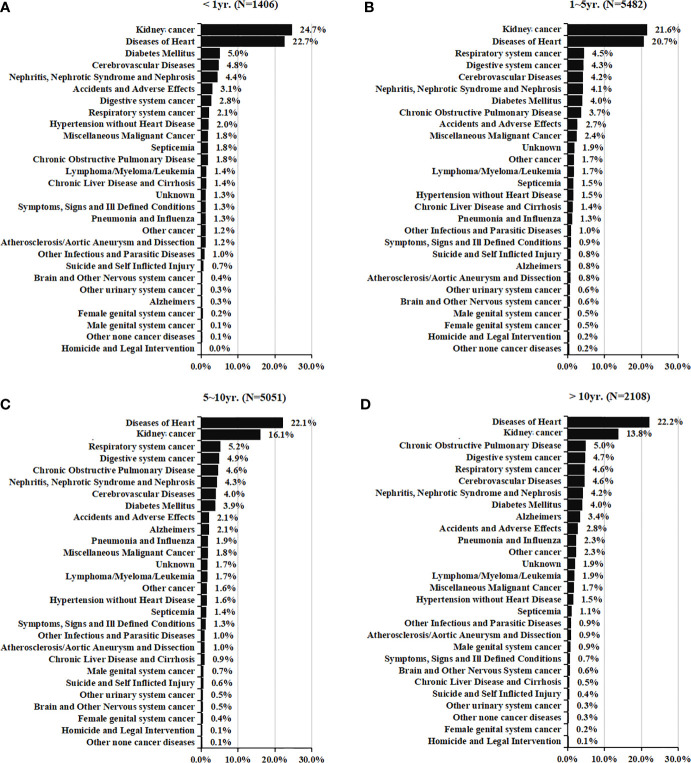
In all, 68,612 eligible patients were pooled. A total of 14,047 (20.5%) patients had died (cardiovascular disease [CVD], 28.3%; other non-cancer-related diseases, 20.3%; RCC, 18.7%; other cancer types, 16.3%; non-disease events, 16.1%) during follow-up. Heart disease, diabetes mellitus, and cerebrovascular disease were the primary causes of non-RCC-related mortality within 1 year after the diagnosis. The greatest proportion of death (39.0%) occurred within 1-5 years after the diagnosis, mostly due to RCC itself, followed by heart disease. However, >5 years after the diagnosis, heart disease became the leading cause of death. Compared with the general US population, a 21% (SMR, 1.21; 95%CI 1.19-1.23) increased risk of all-mortality was observed; RCC patients had a higher risk of heart disease-related death within 5-10 years (SMR, 1.10; 95%CI 1.04-1.17) and >10 years (1.12; 1.02-1.22) after the diagnosis. Older age and RN increased the death risk of CVD and RCC-specific mortality. Although a larger tumor diameter increased the risk of RCC-specific death, this was not a significant predictor for CVD. Moreover, for T1N0M0 RCC tumors of diameter >4 cm, there was no significant difference in CVD incidence for RN PN.
RCC-specific mortality is a common challenge for the prognosis. Importantly, a large proportion and higher SMRs of other non-RCC-related diseases (especially CVD) should not be disregarded for the better holistic management of survivors of local RCC. Targeted prevention strategies for non-RCC-related death could lead to significant reductions in mortality for RCC survivors.
更多的T1N0M0期肾细胞癌(RCC)被检测出来,且预后有所改善,但目前对非RCC相关死亡率的关注较为表面。我们调查了RCC诊断后的死因特异性死亡率及其时间模式。
在监测、流行病学和最终结果-18数据库中,确定2000 - 2015年期间接受部分肾切除术(PN)或根治性肾切除术(RN)治疗的T1N0M0期RCC患者。计算死因的标准化死亡率(SMR)。使用Fine和Gray亚分布模型研究每种死因特异性死亡率的风险预测因素。
总共纳入了68,612例符合条件的患者。在随访期间,共有14,047例(20.5%)患者死亡(心血管疾病[CVD],28.3%;其他非癌症相关疾病,20.3%;RCC,18.7%;其他癌症类型,16.3%;非疾病事件,16.1%)。心脏病、糖尿病和脑血管疾病是诊断后1年内非RCC相关死亡的主要原因。最大比例的死亡(39.0%)发生在诊断后1 - 5年,主要是由于RCC本身,其次是心脏病。然而,诊断后>5年,心脏病成为主要死因。与美国普通人群相比,观察到全因死亡率风险增加21%(SMR,1.21;95%CI 1.19 - 1.23);RCC患者在诊断后5 - 10年(SMR,1.10;95%CI 1.04 - 1.17)和>10年(1.12;1.02 - 1.22)有更高的心脏病相关死亡风险。年龄较大和接受RN增加了CVD和RCC特异性死亡率的死亡风险。虽然肿瘤直径较大增加了RCC特异性死亡风险,但这不是CVD的显著预测因素。此外,对于直径>4 cm的T1N0M0期RCC肿瘤,RN与PN的CVD发病率无显著差异。
RCC特异性死亡率是预后的常见挑战。重要的是,对于局部RCC幸存者的更好的整体管理,不应忽视其他非RCC相关疾病(尤其是CVD)的高比例和更高的SMR。针对非RCC相关死亡的有针对性预防策略可能会显著降低RCC幸存者的死亡率。