Costamagna Andrea, Pivetta Emanuele, Goffi Alberto, Steinberg Irene, Arina Pietro, Mazzeo Anna Teresa, Del Sorbo Lorenzo, Veglia Simona, Davini Ottavio, Brazzi Luca, Ranieri V Marco, Fanelli Vito
Department of Anaesthesia and Critical Care, AOU Città della Salute e della Scienza di Torino, University of Turin, Corso Dogliotti 14, 10126, Turin, Italy.
Department of General and Specialized Medicine, Division of Emergency Medicine and High Dependency Unit, Cancer Epidemiology Unit - AOU Città Della Salute e Della Scienza di Torino, Turin, Italy.
Ann Intensive Care. 2021 Mar 29;11(1):51. doi: 10.1186/s13613-021-00837-1.
To assess diagnostic performance of lung ultrasound (LUS) in identifying ARDS morphology (focal vs non-focal), compared with the gold standard computed tomography.
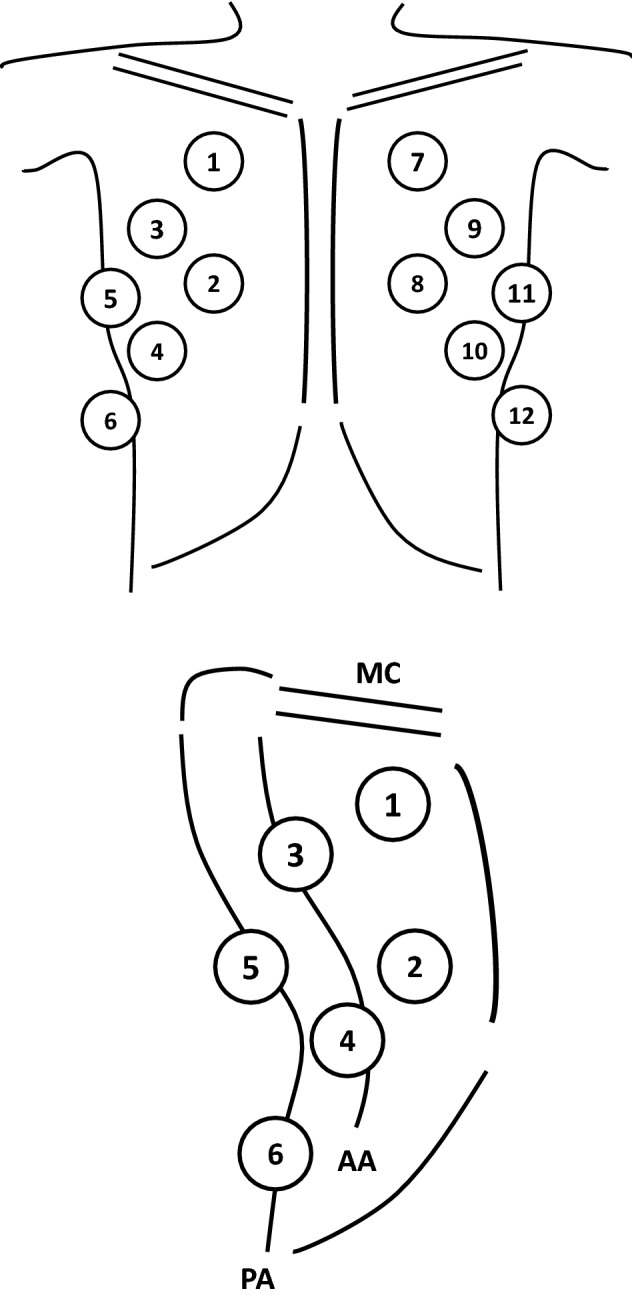
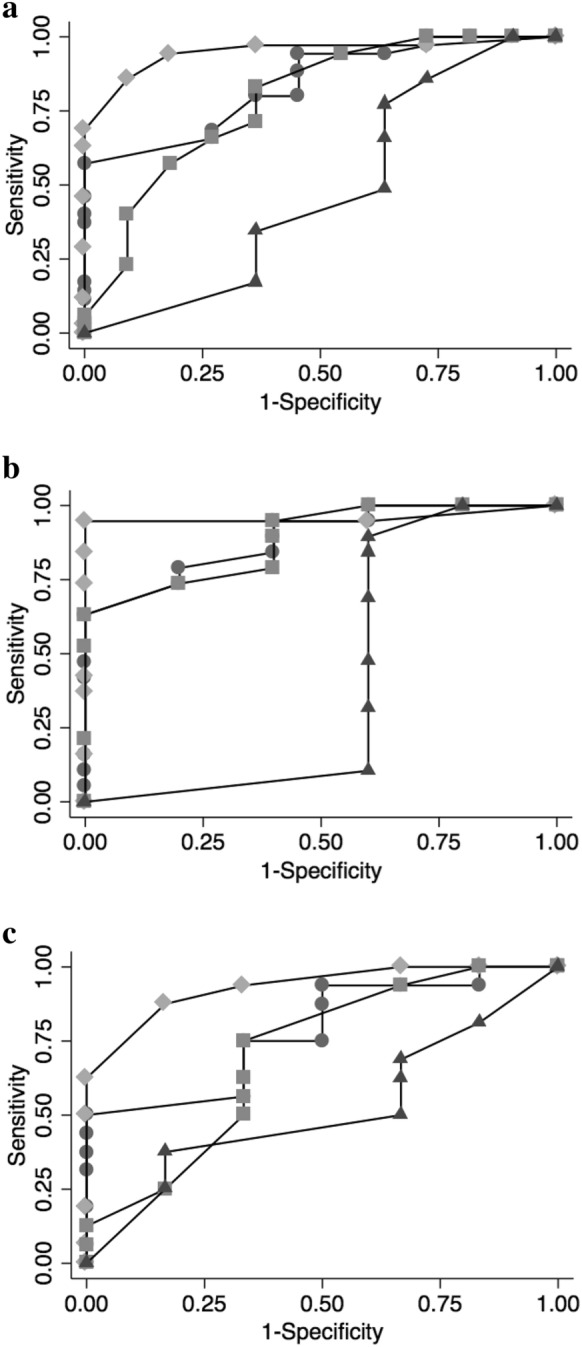
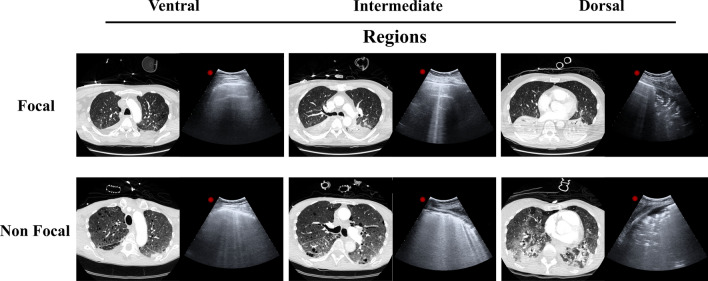
Mechanically ventilated ARDS patients undergoing lung computed tomography and ultrasound were enrolled. Twelve fields, were evaluated. LUS score was graded from 0 (normal) to 3 (consolidation) according to B-lines extent. Total and regional LUS score as the sum of the four ventral (LUS), intermediate (LUS) or dorsal (LUS) fields, were calculated. Based on lung CT, ARDS morphology was defined as (1) focal (loss of aeration with lobar distribution); (2) non-focal (widespread loss of aeration or segmental loss of aeration distribution associated with uneven lung attenuation areas), and diagnostic accuracy of LUS in discriminating ARDS morphology was determined by AU-ROC in training and validation set of patients.
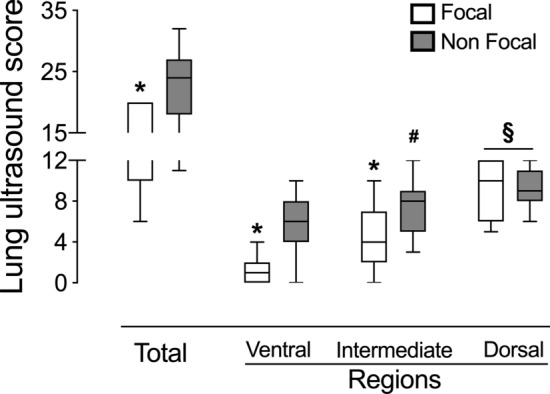
Forty-seven patients with ARDS (25 training set and 22 validation set) were enrolled. LUS, LUS and LUS but not LUS score were significantly lower in focal than in non-focal ARDS morphologies (p < .01). The AU-ROC curve of LUS, LUS, LUS and LUS for identification of non-focal ARDS morphology were 0.890, 0.958, 0.884 and 0.421, respectively. LUS value ≥ 3 had the best predictive value (sensitivity = 0.95, specificity = 1.00) in identifying non-focal ARDS morphology. In the validation set, an LUS score ≥ 3 confirmed to be highly predictive of non-focal ARDS morphology, with a sensitivity and a specificity of 94% and 100%.
LUS had a valuable performance in distinguishing ARDS morphology.
为评估肺部超声(LUS)在识别急性呼吸窘迫综合征(ARDS)形态(局灶性与非局灶性)方面的诊断性能,并与金标准计算机断层扫描进行比较。
纳入接受肺部计算机断层扫描和超声检查的机械通气ARDS患者。评估12个区域。根据B线范围,LUS评分从0(正常)到3(实变)进行分级。计算四个前侧(LUS)、中间(LUS)或后侧(LUS)区域的总和作为总LUS评分和区域LUS评分。基于肺部CT,ARDS形态定义为:(1)局灶性(肺叶分布的通气丧失);(2)非局灶性(广泛的通气丧失或与肺实质不均匀区域相关的节段性通气丧失分布),并通过受试者工作特征曲线下面积(AU-ROC)在患者的训练集和验证集中确定LUS区分ARDS形态的诊断准确性。
纳入47例ARDS患者(25例训练集和22例验证集)。在局灶性ARDS形态中,LUS、LUS和LUS评分但不包括LUS评分显著低于非局灶性ARDS形态(p < 0.0)。LUS、LUS、LUS和LUS用于识别非局灶性ARDS形态的AU-ROC曲线分别为0.890、0.958、0.884和0.421。LUS值≥3在识别非局灶性ARDS形态方面具有最佳预测价值(敏感性 = 0.95,特异性 = 1.00)。在验证集中,LUS评分≥3被证实对非局灶性ARDS形态具有高度预测性,敏感性和特异性分别为94%和100%。
LUS在区分ARDS形态方面具有重要作用。