Fitzhugh Mullan Institute for Health Workforce Equity, The George Washington University Milken Institute School of Public Health, Washington, DC.
Department of Emergency Medicine, The George Washington University School of Medicine and Health Sciences, Washington, DC.
JAMA Netw Open. 2021 Mar 1;4(3):e213789. doi: 10.1001/jamanetworkopen.2021.3789.
The COVID-19 pandemic coupled with health disparities have highlighted the disproportionate burden of disease among Black, Hispanic, and Native American (ie, American Indian or Alaska Native) populations. Increasing transparency around the representation of these populations in health care professions may encourage efforts to increase diversity that could improve cultural competence among health care professionals and reduce health disparities.
To estimate the racial/ethnic diversity of the current health care workforce and the graduate pipeline for 10 health care professions and to evaluate whether the diversity of the pipeline suggests greater representation of Black, Hispanic, and Native American populations in the future.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional study used weighted data from the 2019 American Community Survey (ACS) to compare the diversity of 10 health care occupations (advanced practice registered nurses, dentists, occupational therapists, pharmacists, physical therapists, physician assistants, physicians, registered nurses, respiratory therapists, and speech-language pathologists) with the diversity of the US working-age population, and 2019 data from the Integrated Postsecondary Education Data System (IPEDS) were used to compare the diversity of graduates with that of the US population of graduation age. Data from the IPEDS included all awards and degrees conferred between July 1, 2018, and June 30, 2019, in the US.
A health workforce diversity index (diversity index) was developed to compare the racial/ethnic diversity of the 10 health care professions (or the graduates in the pipeline) analyzed with the racial/ethnic diversity of the current working-age population (or average student-age population). For the current workforce, the index was the ratio of current workers in a health occupation to the total working-age population by racial/ethnic group. For new graduates, the index was the ratio of recent graduates to the population aged 20 to 35 years by racial/ethnic group. A value equal to 1 indicated equal representation of the racial/ethnic groups in the current workforce (or pipeline) compared with the working-age population.
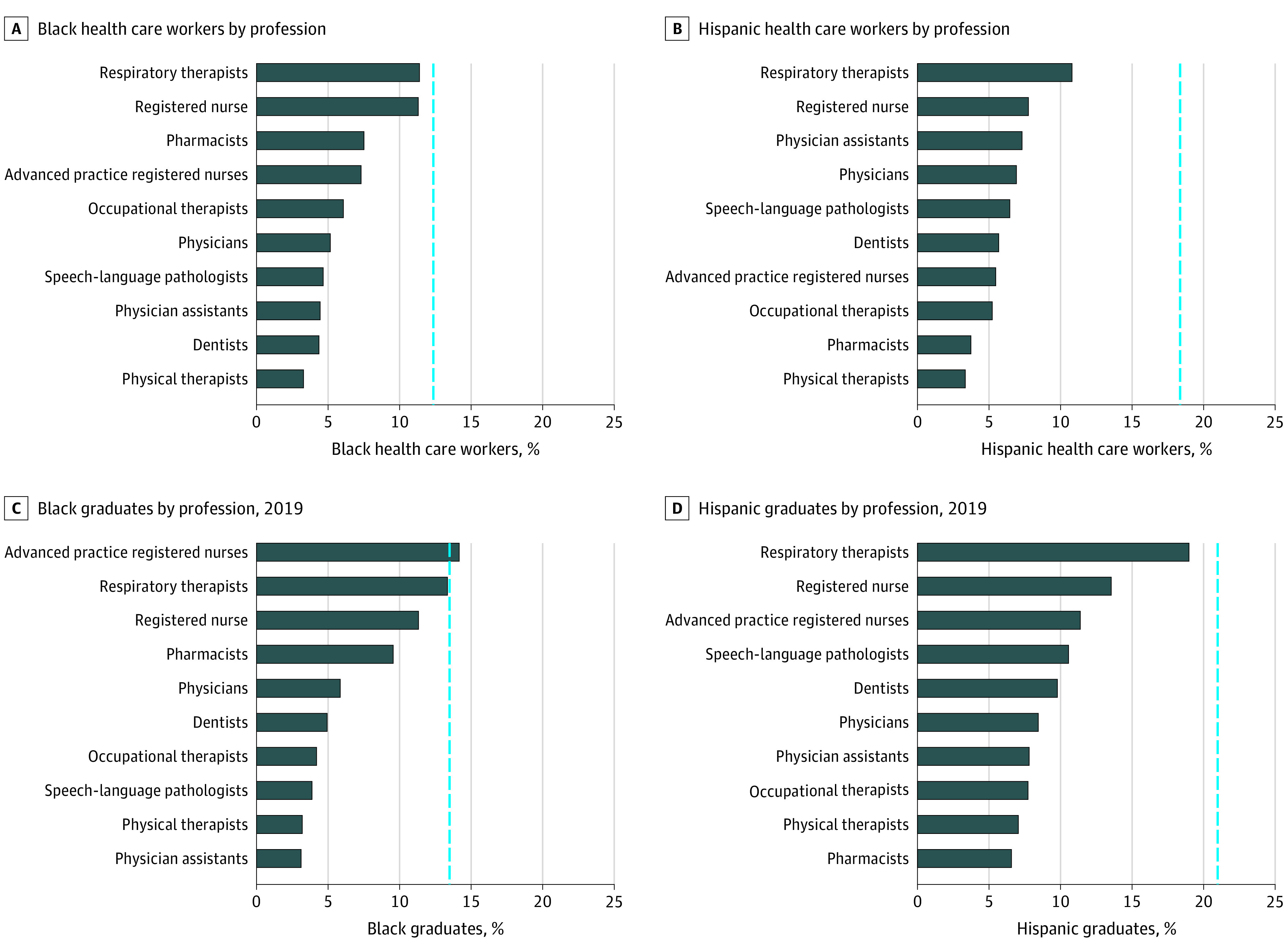
The study sample obtained from the 2019 ACS comprised a weighted total count of 148 358 252 individuals aged 20 to 65 years (White individuals: 89 756 689; Black individuals: 17 916 227; Hispanic individuals: 26 953 648; and Native American individuals: 1 108 404) who were working or searching for work and a weighted total count of 71 608 009 individuals aged 20 to 35 years (White individuals: 38 995 242; Black individuals: 9 830 765; Hispanic individuals: 15 257 274; and Native American individuals: 650 221) in the educational pipeline. Among the 10 professions assessed, the mean diversity index for Black people was 0.54 in the current workforce and in the educational pipeline. In 5 of 10 health care professions, representation of Black graduates was lower than representation in the current workforce (eg, occupational therapy: 0.31 vs 0.50). The mean diversity index for Hispanic people was 0.34 in the current workforce; it improved to 0.48 in the educational pipeline but remained lower than 0.50 in 6 of 10 professions, including physical therapy (0.33). The mean diversity index for Native American people was 0.54 in the current workforce and increased to 0.57 in the educational pipeline.
This study found that Black, Hispanic, and Native American people were underrepresented in the 10 health care professions analyzed. Although some professions had greater diversity than others and there appeared to be improvement among graduates in the educational pipeline compared with the current workforce, additional policies are needed to further strengthen and support a workforce that is more representative of the population.
新冠疫情加上健康差异,突显了黑种人、西班牙裔和美国原住民(即美洲印第安人或阿拉斯加原住民)群体在疾病负担方面的不成比例。增加医疗保健职业中这些人群代表性的透明度,可能会鼓励增加多样性,从而提高医疗保健专业人员的文化能力,并减少健康差异。
估计当前医疗保健劳动力的种族/民族多样性以及 10 种医疗保健职业的研究生管道,并评估该管道的多样性是否表明未来黑人、西班牙裔和美国原住民群体的代表性更高。
设计、设置和参与者:这项横断面研究使用了 2019 年美国社区调查(ACS)的加权数据,将 10 种医疗保健职业(高级执业注册护士、牙医、职业治疗师、药剂师、物理治疗师、医师助理、医生、注册护士、呼吸治疗师和言语语言病理学家)的多样性与美国工作年龄人口的多样性进行比较,并使用 2019 年综合高等教育数据系统(IPEDS)的数据将毕业生的多样性与美国毕业年龄人口的多样性进行比较。IPEDS 中的数据包括 2018 年 7 月 1 日至 2019 年 6 月 30 日期间在美国授予的所有学位。
开发了一个医疗劳动力多样性指数(多样性指数),以比较分析的 10 种医疗保健职业(或管道中的毕业生)的种族/民族多样性与当前工作年龄人口(或平均学生年龄人口)的种族/民族多样性。对于当前劳动力,该指数是健康职业中当前工人与按种族/族裔群体划分的整个工作年龄人口的比率。对于新毕业生,该指数是按种族/族裔群体划分的最近毕业生与 20 至 35 岁年龄人口的比率。等于 1 的值表示与工作年龄人口相比,当前劳动力(或管道)中种族/族裔群体的代表性相等。
从 2019 年 ACS 获得的研究样本包括加权总数为 148358252 名年龄在 20 至 65 岁之间的个人(白人:89756689 人;黑人:17916227 人;西班牙裔:26953648 人;美国原住民:1108404 人),他们正在工作或寻找工作,以及加权总数为 71608009 名年龄在 20 至 35 岁之间的个人(白人:38995242 人;黑人:9830765 人;西班牙裔:15257274 人;美国原住民:650221 人)在教育管道中。在所评估的 10 种职业中,黑人目前劳动力和教育管道中的平均多样性指数为 0.54。在 10 种医疗保健职业中有 5 种,黑人毕业生的代表性低于当前劳动力(例如,职业治疗:0.31 与 0.50)。西班牙裔目前劳动力的平均多样性指数为 0.34;它在教育管道中提高到 0.48,但仍低于 10 种职业中的 0.50,包括物理治疗(0.33)。美国原住民目前劳动力的平均多样性指数为 0.54,在教育管道中增加到 0.57。
这项研究发现,黑种人、西班牙裔和美国原住民在分析的 10 种医疗保健职业中代表性不足。尽管一些职业的多样性高于其他职业,而且与当前劳动力相比,教育管道中的毕业生似乎有所改善,但仍需要采取更多政策,以进一步加强和支持更具代表性的劳动力。