Liver-Kidney Transplantation Unit, Department of Medicine, University of Udine, Udine, Italy.
Hepatobiliary Surgery and Liver Transplantation, University Hospital Pisa, Pisa, Italy.
Updates Surg. 2021 Aug;73(4):1381-1389. doi: 10.1007/s13304-021-01019-1. Epub 2021 Apr 1.
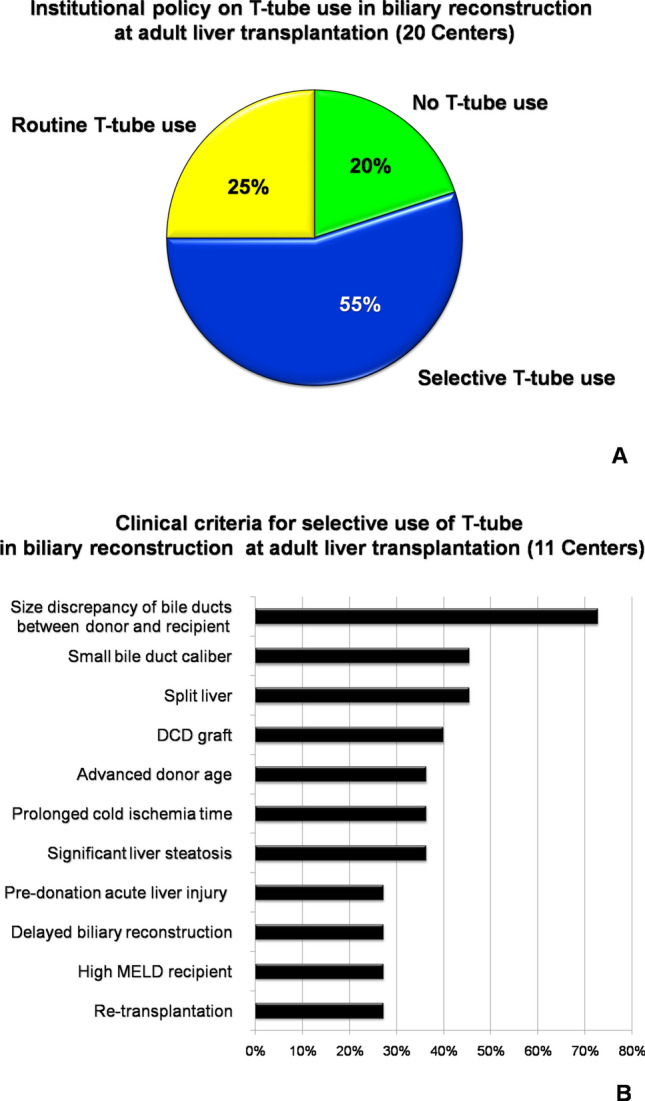
There is enough clinical evidence that a T-tube use in biliary reconstruction at adult liver transplantation (LT) does not significantly modify the risk of biliary stricture/leak, and it may even sustain infective and metabolic complications. Thus, the policy on T-tube use has been globally changing, with progressive application of more restrictive selection criteria. However, there are no currently standardized indications in such change, and many LT Centers rely only on own experience and routine. A nation-wide survey was conducted among all the 20 Italian adult LT Centers to investigate the current policy on T-tube use. It was found that 20% of Centers completely discontinued the T-tube use, while 25% Centers used it routinely in all LT cases. The remaining 55% of Centers applied a selective policy, based on criteria of technical complexity of biliary reconstruction (72.7%), followed by low-quality graft (63.6%) and high-risk recipient (36.4%). A T-tube use > 50% of annual caseload was not associated with high-volume Center status (> 70 LT per year), an active pediatric or living-donor transplant program, or use of DCD grafts. Only 10/20 (50%) Centers identified T-tube as a potential risk factor for complications other than biliary stricture/leak. In these cases, the suspected pathogenic mechanism comprised bacterial colonization (70%), malabsorption (70%), interruption of the entero-hepatic bile-acid cycle (50%), biliary inflammation due to an indwelling catheter (40%) and gut microbiota changes (40%). In conclusion, the prevalence of T-tube use among the Italian LT Centers is still relatively high, compared to the European trend (33%), and the potential detrimental effect of T-tube, beyond biliary stricture/leak, seems to be somehow underestimated.
有足够的临床证据表明,在成人肝移植(LT)中使用 T 管进行胆管重建并不会显著增加胆管狭窄/漏的风险,甚至可能会维持感染和代谢并发症。因此,T 管使用的政策在全球范围内发生了变化,越来越多的选择标准变得更加严格。然而,目前这种变化并没有标准化的适应症,许多 LT 中心仅依赖自身经验和常规。在意大利所有 20 个成人 LT 中心进行了一项全国性调查,以调查目前 T 管使用的政策。结果发现,20%的中心完全停止使用 T 管,而 25%的中心在所有 LT 病例中常规使用 T 管。其余 55%的中心采用了一种选择性的政策,基于胆管重建技术复杂性的标准(72.7%),其次是低质量移植物(63.6%)和高危受者(36.4%)。T 管使用率超过年度病例数的 50%与高容量中心状态(每年超过 70 例 LT)、活跃的儿科或活体供者移植计划或使用 DCD 移植物无关。只有 10/20(50%)的中心将 T 管确定为除胆管狭窄/漏以外的并发症的潜在危险因素。在这些情况下,疑似致病机制包括细菌定植(70%)、吸收不良(70%)、肠肝胆汁酸循环中断(50%)、留置导管引起的胆管炎症(40%)和肠道微生物群变化(40%)。总之,与欧洲趋势(33%)相比,意大利 LT 中心 T 管的使用仍然相对较高,而 T 管除了胆管狭窄/漏之外的潜在有害影响似乎在某种程度上被低估了。