Werlin Evan C, Braun Hillary J, Walker Joy P, Freise Jonathan E, Amara Dominic, Liu Iris H, Mello Anna, Tavakol Mehdi, Stock Peter G, Hiramoto Jade S
Department of Surgery, University of California, San Francisco, San Francisco, CA, United States.
Division of Cardiothoracic and Vascular Surgery, Ohio Health Hospital System, Columbus, OH, United States.
Front Med (Lausanne). 2021 Mar 16;8:606835. doi: 10.3389/fmed.2021.606835. eCollection 2021.
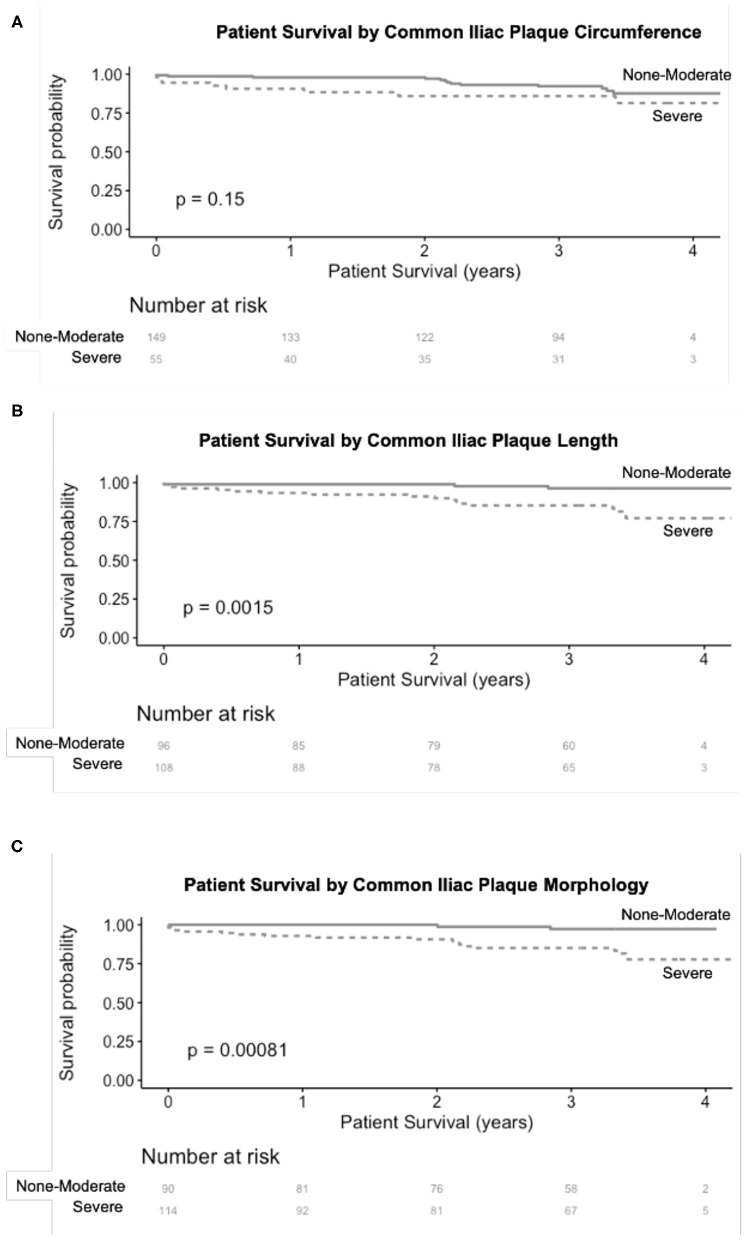
Non-contrast computed tomography scans of the abdomen and pelvis (CTAP) are often obtained prior to renal transplant to evaluate the iliac arteries and help guide surgical implantation. The purpose of this study was to describe the association of iliac calcification scores with operative and clinical outcomes using a simplified scoring system. A retrospective review of 204 patients who underwent renal transplant from 1/2013 to 11/2014 and who had a CTAP within 3 years prior to transplant was performed. Data were collected from the electronic medical record. Common iliac artery (CIA) and external iliac artery (EIA) calcification on CTAP were assessed using a simple scoring system. Descriptive statistics, logistic regression, and survival analyses were performed. A total of 204 patients were included in the analysis. The mean age was 57.4 ± 11.2 years and 134/204 (66%) were men. Nineteen patients (9%) had a history of peripheral artery disease (PAD), 78 (38%) had coronary artery disease, and 22 (11%) had a previous cerebrovascular accident (CVA). Patients with severe right EIA plaque morphology were significantly more likely to require arterial reconstruction compared to those without severe plaque (3/14[21%] 4/153 [3%], = 0.03). Eleven patients (5%) had one or more amputations (toe, foot, or transtibial) following transplant. In UV logistic regression, severe EIA plaque morphology (OR 8.1, CI 2.2-29.6, = 0.002) and PAD (OR 10.7, CI 2.8-39.9, = 0.0004) were associated with increased odds of amputation. In the MV model containing both variables, EIA plaque morphology (OR 4.4, CI 0.99-18.3, = 0.04) and PAD (OR 6.3, CI 1.4-26.4, = 0.01) remained independently associated with increased odds of amputation. Over a median follow up of 3.3 years (IQR 2.9-3.6), 21 patients (10%) had post-operative major adverse cardiac events (MACE, defined as myocardial infarction, coronary intervention, or CVA), and 23 patients died (11%). In unadjusted Kaplan Meier analysis, CIA plaque ( = 0.00081) and >75% CIA length calcification ( = 0.0015) were significantly associated with MACE. Plaque burden in the EIA is associated with increased need for intra-operative arterial reconstruction and post-operative lower extremity amputations, while CIA plaque is associated with post-operative MACE. Assessment of CIA and EIA calcification scores on pre-transplant CT scans in high risk patients may guide operative strategy and perioperative management to improve clinical outcomes.
在肾移植前,通常会进行腹部和盆腔的非增强计算机断层扫描(CTAP),以评估髂动脉情况并辅助指导手术植入。本研究的目的是使用一种简化评分系统描述髂动脉钙化评分与手术及临床结局之间的关联。对2013年1月至2014年11月期间接受肾移植且在移植前3年内进行过CTAP的204例患者进行了回顾性分析。数据从电子病历中收集。使用一种简单评分系统评估CTAP上的髂总动脉(CIA)和髂外动脉(EIA)钙化情况。进行了描述性统计、逻辑回归和生存分析。共有204例患者纳入分析。平均年龄为57.4±11.2岁,134/204(66%)为男性。19例(9%)有外周动脉疾病(PAD)病史,78例(38%)有冠状动脉疾病,22例(11%)有既往脑血管意外(CVA)。与无严重斑块的患者相比,右EIA有严重斑块形态的患者更有可能需要进行动脉重建(3/14[21%]对4/153[3%],P = 0.03)。11例患者(5%)在移植后进行了一次或多次截肢(趾、足或经胫骨截肢)。在单变量逻辑回归中,严重EIA斑块形态(OR 8.1,CI 2.2 - 29.6,P = 0.002)和PAD(OR 10.7,CI 2.8 - 39.9,P = 0.0004)与截肢几率增加相关。在包含这两个变量的多变量模型中,EIA斑块形态(OR 4.4,CI 0.99 - 18.3,P = 0.04)和PAD(OR 6.3,CI 1.4 - 26.4,P = 0.01)仍与截肢几率增加独立相关。在中位随访3.3年(IQR 2.9 - 3.6)期间,21例患者(10%)发生术后主要不良心脏事件(MACE,定义为心肌梗死、冠状动脉介入或CVA),23例患者死亡(11%)。在未调整的Kaplan - Meier分析中,CIA斑块(P = 0.00081)和CIA长度钙化>75%(P = 0.0015)与MACE显著相关。EIA中的斑块负荷与术中动脉重建需求增加及术后下肢截肢相关,而CIA斑块与术后MACE相关。对高危患者移植前CT扫描上的CIA和EIA钙化评分进行评估,可能有助于指导手术策略和围手术期管理,以改善临床结局。