From the Department of Surgery (M.L.M., T.V., R.N.), and Department of Geography (N.W., S.L.L., J.H.), University of Utah, Salt Lake City, Utah.
J Trauma Acute Care Surg. 2021 May 1;90(5):853-860. doi: 10.1097/TA.0000000000003087.
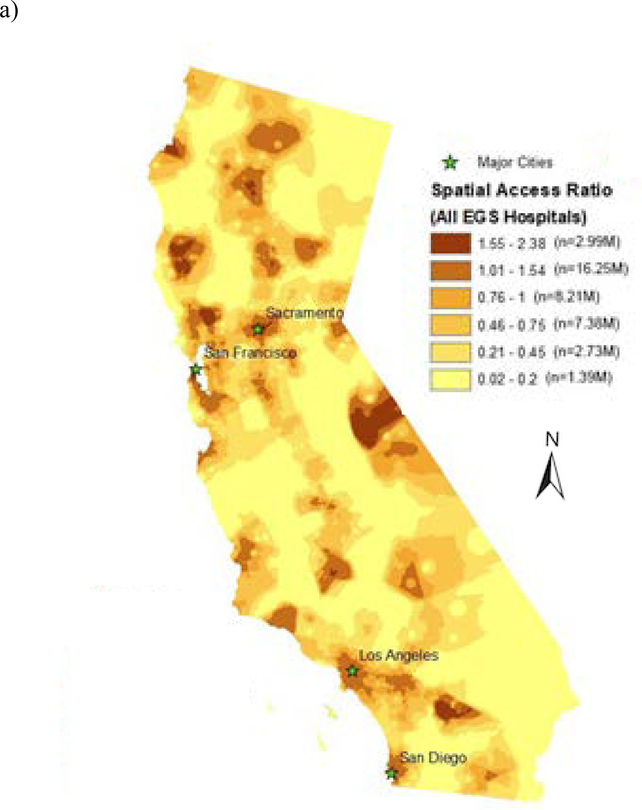
Emergency general surgery (EGS) encompasses a spectrum of time-sensitive and resource-intensive conditions, which require adequate and timely access to surgical care. Developing metrics to accurately quantify spatial access to care is critical for this field. We sought to evaluate the ability of the spatial access ratio (SPAR), which incorporates travel time, hospital capacity, and population demand in its ability to measure spatial access to EGS care and delineate disparities.
We constructed a geographic information science platform for EGS-capable hospitals in California and mapped population location, race, and socioeconomic characteristics. We compared the SPAR to the shortest travel time model in its ability to identify disparities in spatial access overall and for vulnerable populations. Reduced spatial access was defined as >60 minutes travel time or lowest three classes of SPAR.
A total of 283 EGS-capable hospitals were identified, of which 142 (50%) had advanced resources. Using shortest travel time, only 166,950 persons (0.4% of total population) experienced prolonged (>60 minutes) travel time to any EGS-capable hospital, which increased to 1.05 million (2.7%) for advanced-resource centers. Using SPAR, 11.5 million (29.5%) had reduced spatial access to any EGS hospital, and 13.9 million (35.7%) for advanced-resource centers. Rural residents had significantly decreased access for both overall and advanced EGS services when assessed by SPAR despite travel times within the 60-minute threshold.
While travel time and SPAR showed similar overall geographic patterns of spatial access to EGS hospitals, SPAR identified a greater a greater proportion of the population as having limited access to care. Nearly one third of California residents experience reduced spatial access to EGS hospitals when assessed by SPAR. Metrics that incorporate measures of population demand and hospital capacity in addition to travel time may be useful when assessing spatial access to surgical services.
Cross-sectional study, level VI.
急诊普通外科(EGS)涵盖了一系列需要及时获得外科治疗的时间敏感且资源密集型的病症。开发准确衡量医疗资源可及性的指标对于该领域至关重要。我们旨在评估空间可达性比值(SPAR)的能力,该比值将旅行时间、医院容量和人口需求纳入其中,以衡量 EGS 护理的空间可达性并划定差异。
我们构建了一个加利福尼亚州具备 EGS 能力的医院的地理信息科学平台,并绘制了人口位置、种族和社会经济特征。我们比较了 SPAR 与最短旅行时间模型在整体和弱势人群的空间可达性差异识别方面的能力。减少的空间可达性定义为 >60 分钟的旅行时间或 SPAR 的最低三个等级。
共确定了 283 家具备 EGS 能力的医院,其中 142 家(50%)拥有先进资源。使用最短旅行时间,只有 166,950 人(总人口的 0.4%)到任何 EGS 能力的医院的旅行时间超过 60 分钟,对于拥有先进资源的中心而言,这一数字增加到 105 万人(2.7%)。使用 SPAR,有 1150 万人(29.5%)到任何 EGS 医院的空间可达性降低,而对于拥有先进资源的中心,这一数字为 1390 万人(35.7%)。尽管旅行时间在 60 分钟的范围内,但农村居民在 SPAR 评估的整体和高级 EGS 服务方面的可达性明显降低。
虽然旅行时间和 SPAR 显示出 EGS 医院空间可达性的整体地理模式相似,但 SPAR 确定了更多的人难以获得医疗服务。当通过 SPAR 评估时,近三分之一的加利福尼亚居民的 EGS 医院的空间可达性降低。在评估手术服务的空间可达性时,除旅行时间外,纳入人口需求和医院容量的指标可能会很有用。
横断面研究,六级。