Department of Gynecology and Obstetrics, Breast and Gynecologic Cancer Center, Marienhospital, Josef-Albers-Str. 70, 46236, Bottrop, Germany.
Department of Obstetrics and Gynecology, Breast and Gynecologic Cancer Center, Sana Klinikum Offenbach, Starkenburgring 66, D-63069, Offenbach, Germany.
Breast. 2021 Jun;57:95-103. doi: 10.1016/j.breast.2021.03.003. Epub 2021 Mar 18.
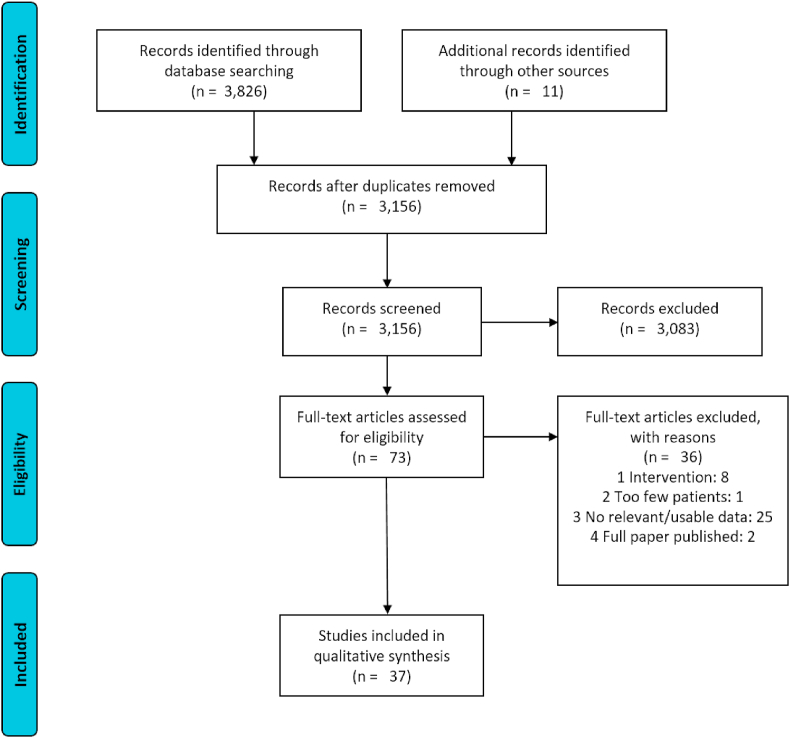
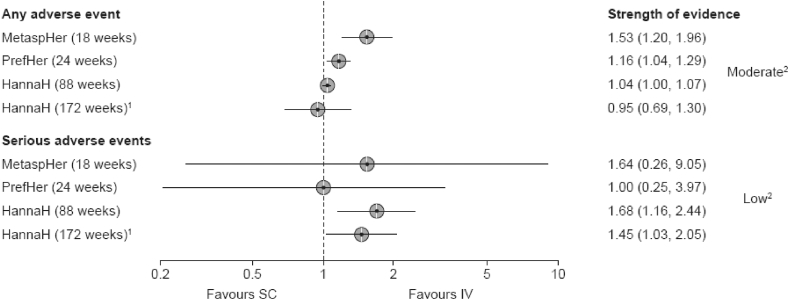
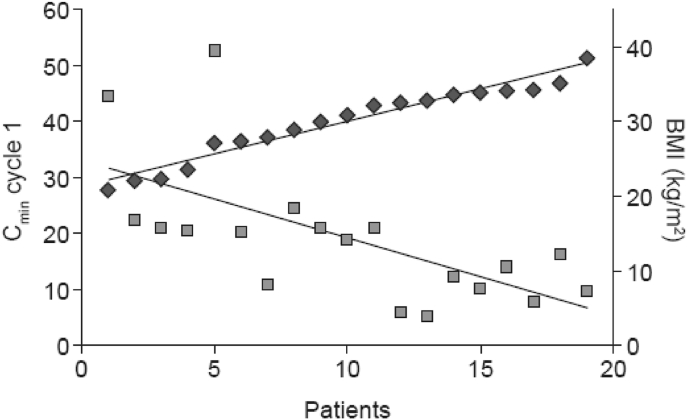
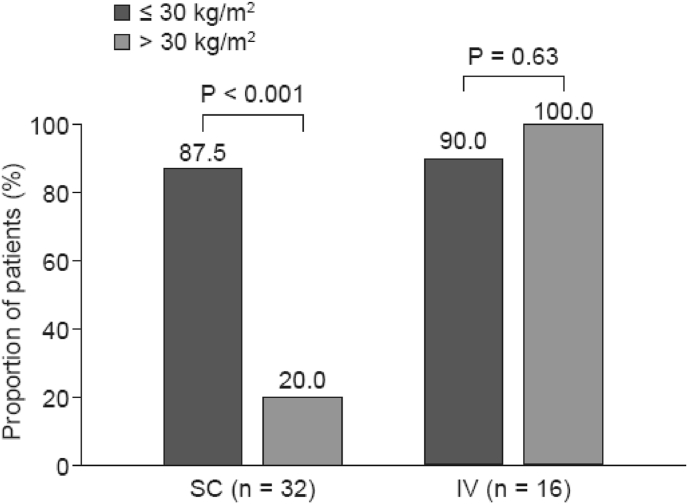
Trastuzumab, a key treatment for HER2-positive breast cancer, is available in weight-based IV and fixed-dose (600 mg) SC formulations. While the Phase 3 HannaH trial indicated non-inferiority of the SC formulation, there is some concern that the target plasma concentration may not be reached in overweight/obese patients whereas low-body-weight patients may be at risk of toxicity. This scoping review evaluated whether overweight/obese patients are at risk of below-target exposure with fixed-dose SC trastuzumab, whether low-body-weight patients are at risk of increased toxicity, especially cardiotoxicity, and whether IV and SC trastuzumab are equivalent in terms of treatment-emergent adverse events (TEAEs) (e.g. infections). Thirty-seven publications that met the eligibility criteria were included. Body weight is not an important determinant of exposure to trastuzumab at steady state (i.e. pre-dose cycle 8); however, real-world evidence suggests that the target concentration (20 μg/mL) may not be reached with the first SC dose in overweight/obese patients. There is no evidence that low-body-weight patients are at increased risk of cardiotoxicity with SC trastuzumab, although this may be confounded by the higher rate of cardiovascular comorbidities in overweight patients. In Phase 3 trials, SC trastuzumab was associated with higher rates of ISRs, ADAs and SAEs, the latter often requiring hospitalization and occurring during adjuvant treatment when patients are not burdened by chemotherapy. The route of administration of trastuzumab (IV vs SC) in different treatment settings should be discussed with the patient, taking into account the risks and benefits associated with each route.
曲妥珠单抗是治疗 HER2 阳性乳腺癌的重要药物,有基于体重的静脉注射和固定剂量(600 毫克)皮下注射两种剂型。虽然 III 期 HannaH 试验表明皮下注射剂型具有非劣效性,但有人担心超重/肥胖患者的目标血浆浓度可能无法达到,而低体重患者可能有发生毒性的风险。本范围界定综述评估了固定剂量皮下注射曲妥珠单抗是否会使超重/肥胖患者面临目标暴露不足的风险,低体重患者是否有发生毒性(如心脏毒性)增加的风险,以及静脉注射和皮下注射曲妥珠单抗在治疗相关不良事件(TEAEs)(如感染)方面是否等效。符合入选标准的 37 篇文献被纳入。体重不是稳定状态(即第 8 个周期前剂量)下曲妥珠单抗暴露的重要决定因素;然而,实际证据表明,超重/肥胖患者首次皮下注射时可能无法达到目标浓度(20μg/ml)。没有证据表明低体重患者接受皮下注射曲妥珠单抗时心脏毒性风险增加,尽管这可能因超重患者心血管合并症发生率较高而受到影响。在 III 期试验中,与静脉注射曲妥珠单抗相比,皮下注射曲妥珠单抗更常导致注射部位反应、抗药抗体和严重不良事件,后者通常需要住院治疗,并且发生在辅助治疗期间,此时患者不受化疗的负担。应根据每种给药途径的风险和获益,与患者讨论曲妥珠单抗的给药途径(静脉注射与皮下注射)在不同治疗环境下的选择。