Jünger Stephanie T, Pennig Lenhard, Schödel Petra, Goldbrunner Roland, Friker Lea, Kocher Martin, Proescholdt Martin, Grau Stefan
Centre for Neurosurgery, Department of General Neurosurgery, Faculty of Medicine and University Hospital Cologne, University of Cologne, 50923 Cologne, Germany.
Centre for Integrated Oncology, Faculty of Medicine and University Hospital Cologne, University of Cologne, 50923 Cologne, Germany.
Cancers (Basel). 2021 Mar 21;13(6):1435. doi: 10.3390/cancers13061435.
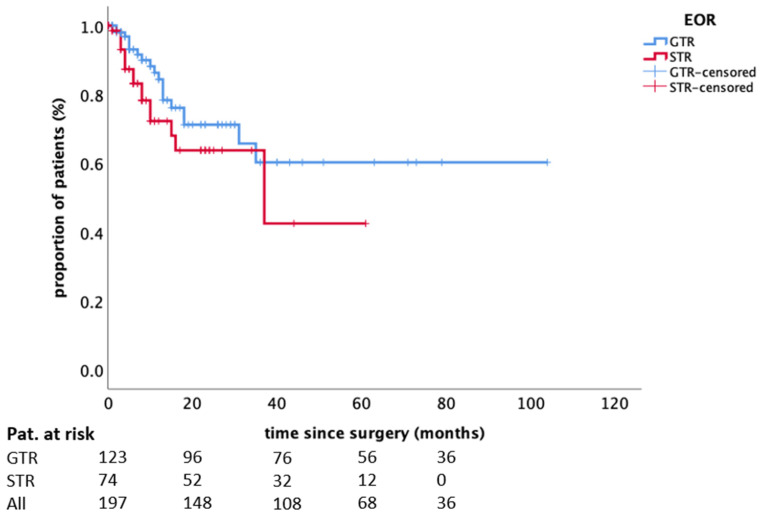
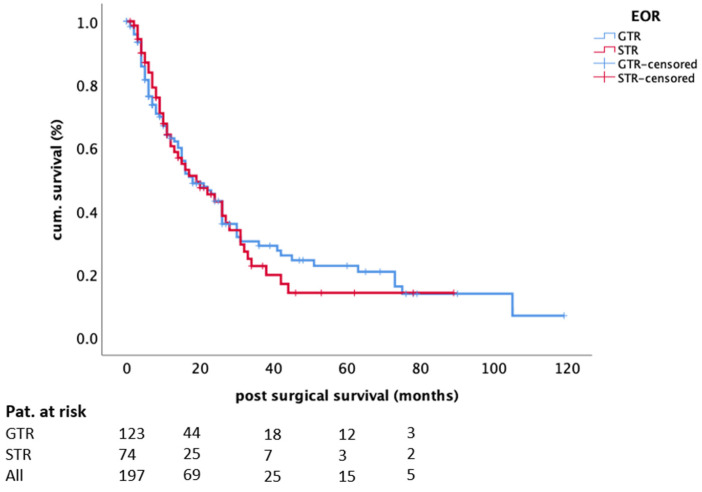
The value of gross-total surgical resection remains debatable in patients with brain metastases (BMs) as most patients succumb to systemic disease progression. In this study, we evaluated the impact of the extent of resection of singular/solitary BM on in-brain recurrence (iBR), focusing on local recurrence (LR) and overall survival (OS) in an interdisciplinary adjuvant treatment setting. In this monocentric retrospective analysis, we included patients receiving surgery of one BM and subsequent adjuvant treatment. A radiologist and a neurosurgeon determined in consensus the extent of resection based on magnetic resonance imaging. The OS was calculated using Kaplan-Meier estimates; prognostic factors for LR and OS were analysed by Log rank test and Cox proportional hazards. We analyzed 197 patients. Gross-total resection was achieved in 123 (62.4%) patients. All patients were treated with adjuvant radiotherapy, and 130 (66.0%) received systemic treatment. Ninety-six (48.7%) patients showed iBR with an LR rate of 23.4%. LR was not significantly influenced by the extent of resection ( = 0.139) or any other parameter. The median OS after surgery was 18 (95%CI 12.5-23.5) months. In univariate analysis, the extent of resection did not influence OS ( = 0.6759), as opposed to adjuvant systemic treatment ( < 0.0001) and controlled systemic disease ( = 0.039). Systemic treatment and controlled disease status remained independent factors for OS ( < 0.0001 and = 0.009, respectively). In this study, the extent of resection of BMs neither influenced the LR nor the OS of patients receiving interdisciplinary adjuvant treatment.
对于脑转移瘤(BMs)患者,手术全切的价值仍存在争议,因为大多数患者死于全身疾病进展。在本研究中,我们评估了单个/孤立性BM切除范围对脑内复发(iBR)的影响,重点关注多学科辅助治疗背景下的局部复发(LR)和总生存期(OS)。在这项单中心回顾性分析中,我们纳入了接受单个BM手术及后续辅助治疗的患者。一名放射科医生和一名神经外科医生根据磁共振成像共同确定切除范围。采用Kaplan-Meier估计法计算OS;通过对数秩检验和Cox比例风险模型分析LR和OS的预后因素。我们分析了197例患者。123例(62.4%)患者实现了手术全切。所有患者均接受了辅助放疗,130例(66.0%)接受了全身治疗。96例(48.7%)患者出现iBR,LR率为23.4%。LR未受切除范围(P = 0.139)或任何其他参数的显著影响。术后中位OS为18(95%CI 12.5 - 23.5)个月。在单因素分析中,切除范围未影响OS(P = 0.6759),与辅助全身治疗(P < 0.0001)和可控的全身疾病(P = 0.039)情况相反。全身治疗和疾病控制状态仍是OS的独立因素(分别为P < 0.0001和P = 0.009)。在本研究中,BMs的切除范围既未影响接受多学科辅助治疗患者的LR,也未影响其OS。