Department of Radiation Oncology, Inselspital, Bern University Hospital and University of Bern, Freiburgstrasse 18, CH-3010, Bern, Switzerland.
Department of Neurosurgery, Inselspital, Bern University Hospital and University of Bern, Bern, Switzerland.
Radiat Oncol. 2019 Mar 14;14(1):45. doi: 10.1186/s13014-019-1252-x.
Administering stereotactic radiotherapy to the surgical cavity and thus omitting postoperative whole brain radiotherapy (WBRT) is a favored strategy in limited metastatic brain disease. Little is known about the impact of regular magnetic resonance imaging follow-up (MRI FU) in such patient cohorts. The aim of this study is to examine the impact of regular MRI FU and to report the oncological outcomes of patients with one to three brain metastases (BMs) treated with stereotactic radiosurgery (SRS) or hypo-fractionated stereotactic radiotherapy (HFSRT) to the surgical cavity.
We retrospectively analyzed patients who received SRS or HFSRT to the surgical cavity after resection of one to two BMs. Additional, non-resected BMs were managed with SRS alone. Survival was estimated by the Kaplan-Meier method. Prognostic factors were examined with the log-rank test and Cox proportional hazards model. Regular MRI FU was defined as performing a brain MRI 3 months after radiotherapy (RT) and/or performing ≥1 brain MRI per 180 days. Primary endpoint was local control (LC). Secondary endpoints were distant brain control (DBC), overall survival (OS) and the correlation between regular MRI FU and overall survival (OS), symptom-free survival (SFS), deferment of WBRT and WBRT-free survival (WFS).
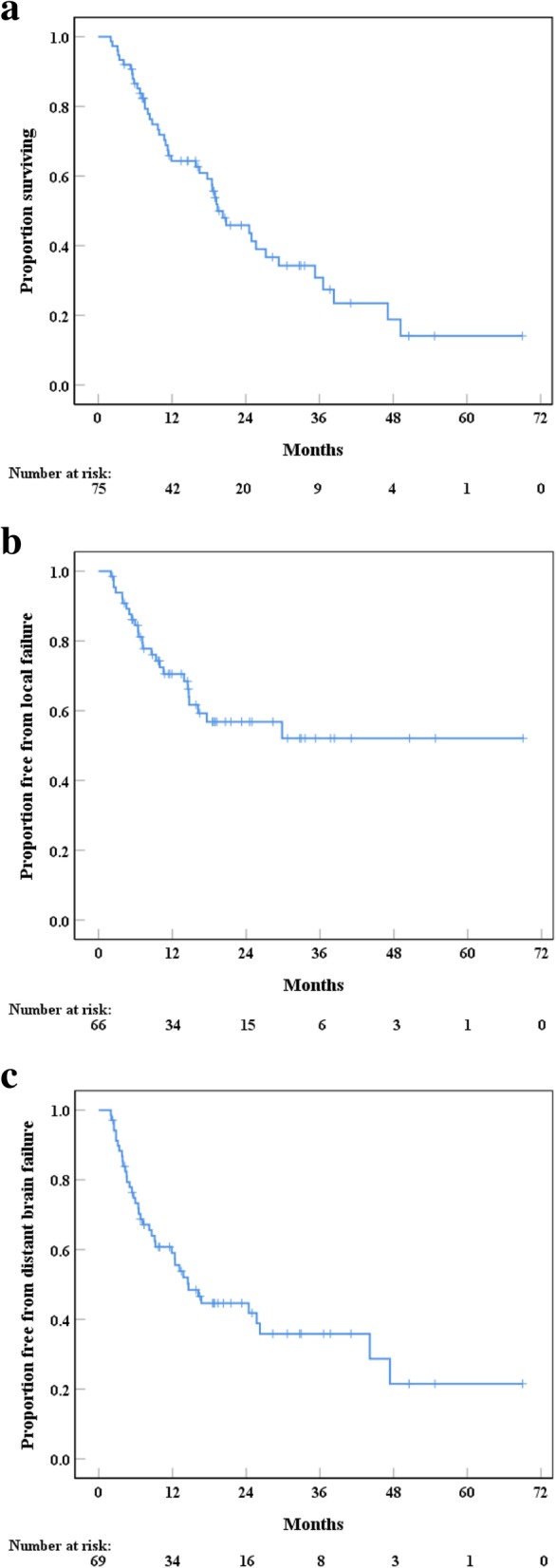
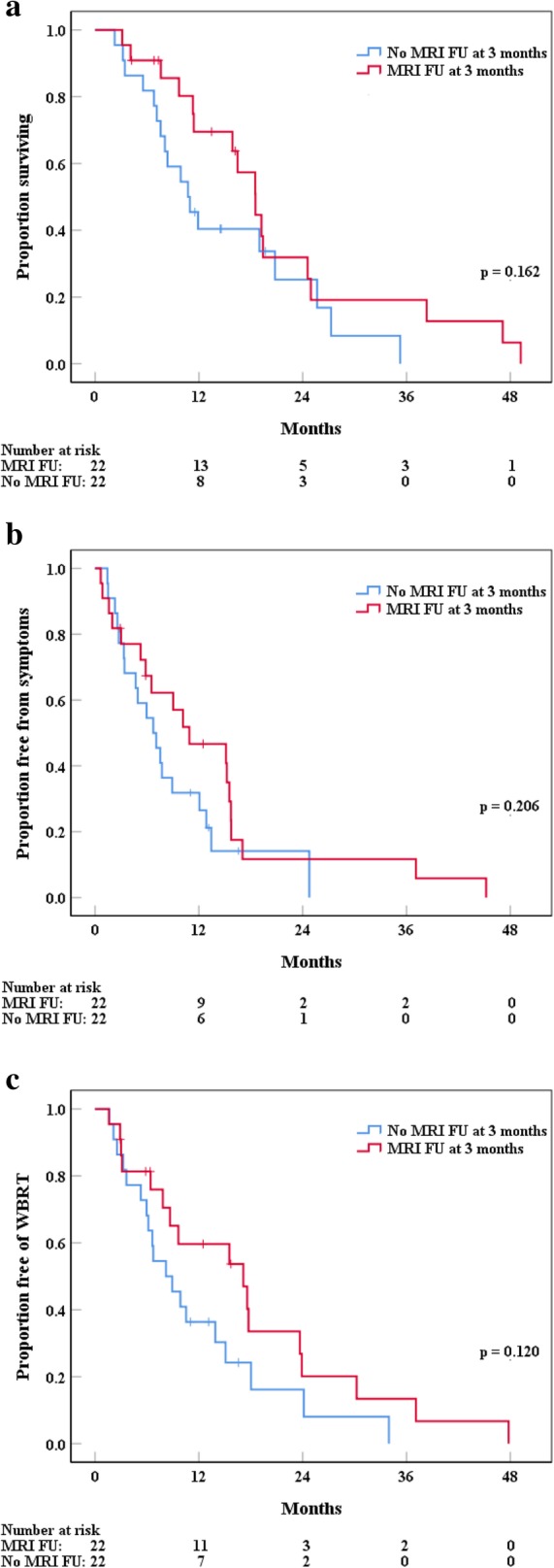
Overall, 75 patients were enrolled. One, 2 and 3 BMs were seen in 63 (84%), 11 (15%) and 1 (1%) patients, respectively. Forty (53%) patients underwent MRI FU 3 months after RT and 38 (51%) patients received ≥1 brain MRI per 180 days. Median OS was 19.4 months (95% CI: 13.2-25.6 months). Actuarial LC, DBC and OS at 1 year were 72% (95% CI: 60-83%), 60% (95% CI: 48-72%) and 66% (95% CI: 53-76%), respectively. A planning target volume > 15 cm (p = 0.01), Graded Prognostic Assessment (GPA) score (p = 0.001) and residual tumor after surgery (p = 0.008) were prognostic for decreased OS in multivariate analysis. No significant correlation between MRI FU at 3 months and OS (p = 0.462), SFS (p = 0.536), WFS (p = 0.407) or deferment of WBRT (p = 0.955) was seen. Likewise, performing ≥1 MRI per 180 days had no significant impact on OS (p = 0.954), SFS (p = 0.196), WFS (p = 0.308) or deferment of WBRT (p = 0.268).
Our results regarding oncological outcomes consist with the current data from the literature. Surprisingly, regular MRI FU did not result in increased OS, SFS, WFS or deferment of WBRT in our cohort consisting mainly of patients with a single and resected BM. Therefore, the impact of regular MRI FU needs prospective evaluation.
Project ID: 2017-00033, retrospectively registered.
在有限的转移性脑疾病中,向手术腔给予立体定向放射治疗并因此省略术后全脑放疗(WBRT)是一种受青睐的策略。对于这种患者群体,常规磁共振成像随访(MRI FU)的影响知之甚少。本研究旨在检查常规 MRI FU 的影响,并报告接受立体定向放射外科(SRS)或低分割立体定向放射治疗(HFSRT)治疗 1 至 3 个脑转移瘤(BMs)的患者的肿瘤学结果。
我们回顾性分析了接受手术后 1 至 2 个 BMs 的 SRS 或 HFSRT 治疗的患者。另外,单独用 SRS 治疗非切除的 BMs。通过 Kaplan-Meier 法估计生存。用对数秩检验和 Cox 比例风险模型检查预后因素。常规 MRI FU 定义为在放疗(RT)后 3 个月进行脑部 MRI 检查和/或每 180 天进行≥1 次脑部 MRI。主要终点为局部控制(LC)。次要终点为远处脑控制(DBC)、总生存(OS)以及常规 MRI FU 与总生存(OS)、症状无进展生存(SFS)、WBRT 推迟和 WBRT 无进展生存(WFS)之间的相关性。
总体而言,共有 75 名患者入组。63 名(84%)患者有 1 个、11 名(15%)患者有 2 个和 1 名(1%)患者有 3 个 BMs。40 名(53%)患者在 RT 后 3 个月接受 MRI FU,38 名(51%)患者每 180 天接受≥1 次脑部 MRI。中位 OS 为 19.4 个月(95%CI:13.2-25.6 个月)。1 年时的累积 LC、DBC 和 OS 分别为 72%(95%CI:60-83%)、60%(95%CI:48-72%)和 66%(95%CI:53-76%)。多变量分析显示,计划靶体积>15 cm(p=0.01)、分级预后评估(GPA)评分(p=0.001)和手术后残余肿瘤(p=0.008)与 OS 降低相关。在 3 个月时进行 MRI FU 与 OS(p=0.462)、SFS(p=0.536)、WFS(p=0.407)或 WBRT 推迟(p=0.955)之间无显著相关性。同样,每 180 天进行≥1 次 MRI 检查对 OS(p=0.954)、SFS(p=0.196)、WFS(p=0.308)或 WBRT 推迟(p=0.268)也没有显著影响。
我们关于肿瘤学结果的研究结果与目前文献中的数据一致。令人惊讶的是,在我们主要由单个和切除的 BM 患者组成的队列中,常规 MRI FU 并未导致 OS、SFS、WFS 或 WBRT 推迟的增加。因此,常规 MRI FU 的影响需要前瞻性评估。
项目 ID:2017-00033,回顾性注册。