Koulouris Charilaos, Paraschou Aristoklis, Manaki Vasiliki, Mantalovas Stylianos, Spiridou Kassiani, Spiridou Andreana, Laskou Styliani, Michalopoulos Nickos, Radu Petru Adrian, Cartu Dan, Șurlin Valeriu, Strambu Victor, Kesisoglou Isaak, Sapalidis Konstantinos
3rd Surgery Department, Medical School of Health Sciences, AHEPA University Hospital, Aristotle University of Thessaloniki, 54636 Thessaloniki, Greece.
Department of Surgery, University of Medicine and Pharmacy Carol Davila Bucharest, 020021 București, Romania.
Medicina (Kaunas). 2021 Mar 24;57(4):303. doi: 10.3390/medicina57040303.
Substernal goiter is usually defined as a goiter that extends below the thoracic inlet or a goiter with more than 50% of its mass lying below the thoracic inlet. Substernal goiters may compress adjacent anatomical structures causing a variety of symptoms.
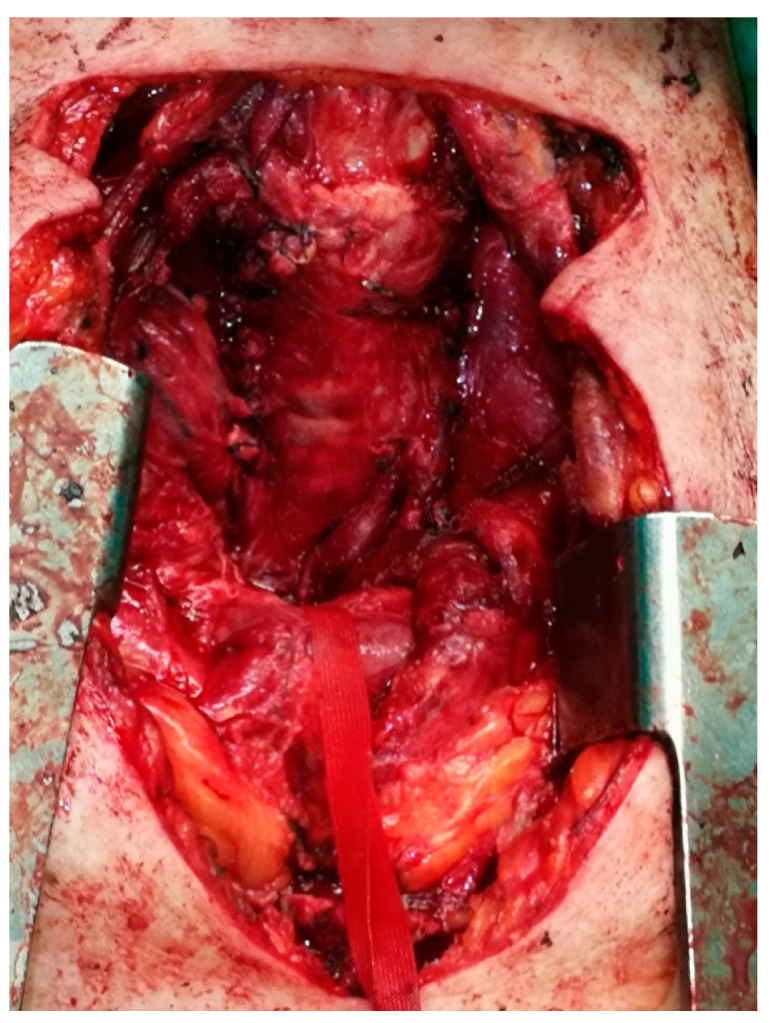
Here we report a rare case of a 75-year-old woman presenting with cardiac arrest caused by acute respiratory failure due to tracheal compression by a substernal goiter.
Substernal goiters can be classified as primary or secondary depending on their site of origin. Symptoms are diverse and include a palpable neck mass, mild dyspnea to asphyxia, dysphagia, dysphonia, and superior vena cava syndrome. Diagnosis of substernal goiter is largely based on computed tomography imaging, which will show the location of the goiter and its extension in the thoracic cavity. Surgery is the treatment of choice for symptomatic patients with substernal goiter. The majority of substernal goiters are resected through a cervical approach. However, in approximately 5% of patients, a thoracic approach is required. The most important factor determining whether a thoracic approach should be used is the depth of the extension to the tracheal bifurcation on CT imaging.
Cardiac arrest appearing as the first symptom of a substernal goiter is a very rare condition and should be treated by emergency thyroidectomy via a cervical or thoracic approach depending on the CT imaging findings.
胸骨后甲状腺肿通常定义为延伸至胸廓入口以下的甲状腺肿,或其肿块超过50%位于胸廓入口以下的甲状腺肿。胸骨后甲状腺肿可能压迫相邻解剖结构,导致各种症状。
我们在此报告一例罕见病例,一名75岁女性因胸骨后甲状腺肿压迫气管导致急性呼吸衰竭,进而引发心脏骤停。
胸骨后甲状腺肿可根据其起源部位分为原发性或继发性。症状多样,包括可触及的颈部肿块、从轻度呼吸困难到窒息、吞咽困难、声音嘶哑以及上腔静脉综合征。胸骨后甲状腺肿的诊断主要基于计算机断层扫描成像,该成像可显示甲状腺肿的位置及其在胸腔内的延伸情况。对于有症状的胸骨后甲状腺肿患者,手术是首选治疗方法。大多数胸骨后甲状腺肿通过颈部入路切除。然而,约5%的患者需要采用胸部入路。决定是否采用胸部入路的最重要因素是计算机断层扫描成像上甲状腺肿延伸至气管分叉处的深度。
以心脏骤停作为胸骨后甲状腺肿的首发症状是一种非常罕见的情况,应根据计算机断层扫描成像结果,通过颈部或胸部入路进行急诊甲状腺切除术。