Achenbach Jannis, Saft Carsten, Faissner Simon
Huntington Center North Rhine-Westphalia, Department of Neurology, Ruhr-University Bochum, St. Josef-Hospital Bochum, Gudrunstraße 56, 44791 Bochum, Germany.
Brain Sci. 2021 Mar 25;11(4):413. doi: 10.3390/brainsci11040413.
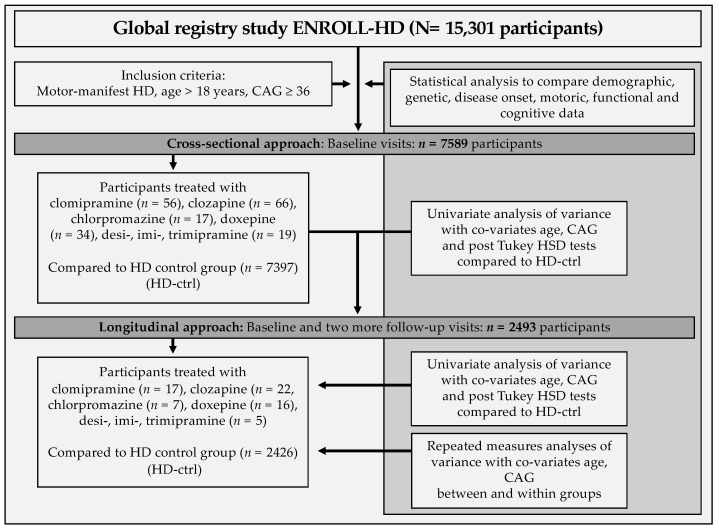
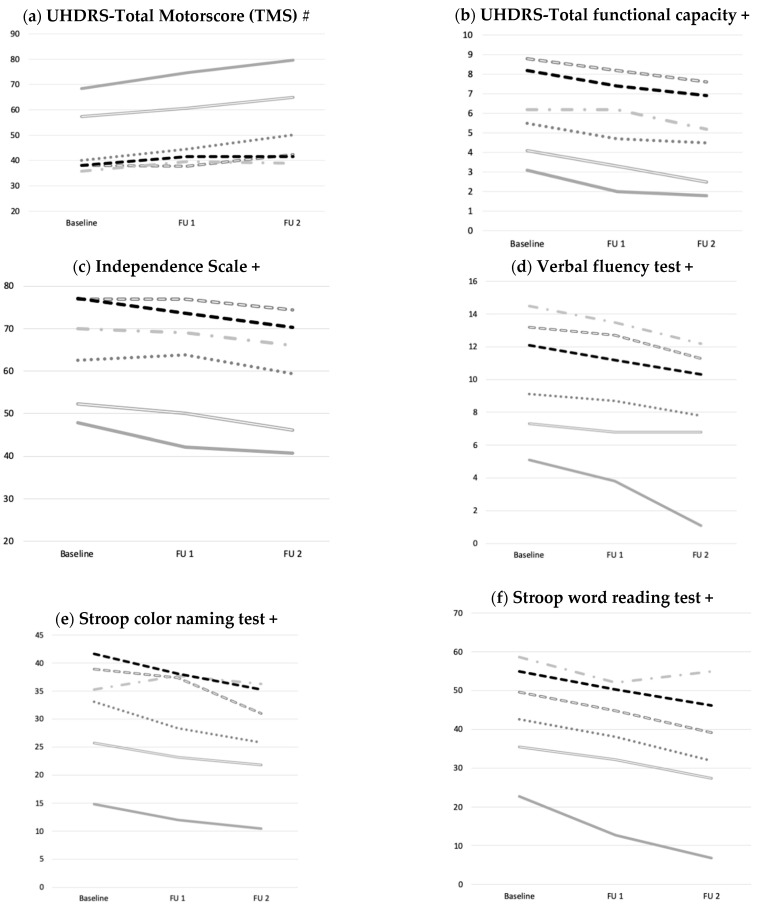
Reducing the progress of neurodegeneration is a key goal in Huntington´s disease (HD). A previously performed systematic screening for medications with neuroprotective features identified tricyclic antidepressants and neuroleptics as neuroprotective and mitochondrioprotective agents. Here, we analyzed the characteristics of disease manifestation, progression and potential beneficial effects in HD patients treated with afore-mentioned medications compared to un- and otherwise treated motor-manifest patients in a large real-world cohort over two years. We analyzed cross-sectional data of the largest cohort worldwide of motor-manifest HD patients using the ENROLL-HD database, including demographic, moleculargenetic, clinical-motoric, cognitive and functional data. Longitudinal data of up to two years were obtained to analyze potential effects on disease progression between groups with different medications used. Data were analyzed using repeated ANOVA-analyses while controlling for the co-variates age and CAG-repeat length. We identified = 7397 motor-manifest HD patients using no or different medication (HD-ctrl) and subgroups treated with clomipramine ( = 56), clozapine ( = 66), chlorpromazine ( = 17), doxepine ( = 34) and desi-, imi- or trimipramine ( = 19). Demographic parameters, disease onset and CAP-score did not differ. Total motor scores (TMS) at baseline were higher in patients treated with clozapine ( < 0.001), chlorpromazine and clomipramine ( < 0.05) compared to HD-ctrl with higher sub scores for bradykinesia (all < 0.01) and dystonia in clozapine treated patients ( < 0.001). Functional and cognitive capacities were worse in medication groups in comparison to HD-ctrl at baseline ( < 0.001). Repeated measures analysis of variance documented no differences regarding motoric, functional and cognitive disease progressions between groups. We identified group differences, potentially caused by side effects or potential selection bias in terms of bradykinetic motoric symptoms, more dystonia and lower functional and cognitive performance in some treatment groups at baseline, which were not entirely explained because of underlying fundamental characteristics. Disease progression regarding clinical, functional and cognitive outcomes over two years was not affected by any of the treatment groups compared to HD-ctrl. Our data do not support our hypothesis of a potential neuroprotective effect of these drugs on disease progression.
减缓神经退行性变进程是亨廷顿舞蹈病(HD)的一个关键目标。先前对具有神经保护特性的药物进行的系统筛查确定三环类抗抑郁药和抗精神病药物为神经保护和线粒体保护剂。在此,我们分析了在一个大型真实世界队列中,与未接受治疗及接受其他治疗的运动症状明显的患者相比,接受上述药物治疗的HD患者的疾病表现、进展特征及潜在有益效果,研究为期两年。我们使用ENROLL-HD数据库分析了全球最大的运动症状明显的HD患者队列的横断面数据,包括人口统计学、分子遗传学、临床运动学、认知和功能数据。获取了长达两年的纵向数据,以分析不同用药组之间对疾病进展的潜在影响。在控制年龄和CAG重复长度等协变量的同时,使用重复方差分析对数据进行分析。我们确定了7397名未用药或使用不同药物的运动症状明显的HD患者(HD对照组),以及接受氯米帕明(56例)、氯氮平(66例)、氯丙嗪(17例)、多塞平(34例)和去甲替林、丙咪嗪或曲米帕明(19例)治疗的亚组。人口统计学参数、疾病发作和CAP评分无差异。与HD对照组相比,接受氯氮平治疗的患者(P<0.001)、氯丙嗪和氯米帕明治疗的患者(P<0.05)基线时的总运动评分(TMS)更高,氯氮平治疗的患者运动迟缓(均P<0.01)和肌张力障碍的分项评分更高(P<0.001)。与HD对照组相比,用药组在基线时的功能和认知能力更差(P<0.001)。重复测量方差分析表明,各组之间在运动、功能和认知疾病进展方面无差异。我们发现了组间差异,可能是由副作用或潜在的选择偏倚导致的,表现为某些治疗组在基线时存在运动迟缓症状、更多的肌张力障碍以及更低的功能和认知表现,由于潜在的基本特征,这些差异并未得到完全解释。与HD对照组相比,两年内任何治疗组对临床、功能和认知结局的疾病进展均无影响。我们的数据不支持这些药物对疾病进展具有潜在神经保护作用的假设。