D'Aiello Angelica, Lin Juan, Gucalp Rasim, Tabatabaie Vafa, Cheng Haiying, Bloomgarden Noah A, Tomer Yaron, Halmos Balazs
Department of Medicine, Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, NY 10467, USA.
Department of Epidemiology and Population Health, Albert Einstein College of Medicine, Bronx, NY 10461, USA.
Cancers (Basel). 2021 Mar 23;13(6):1464. doi: 10.3390/cancers13061464.
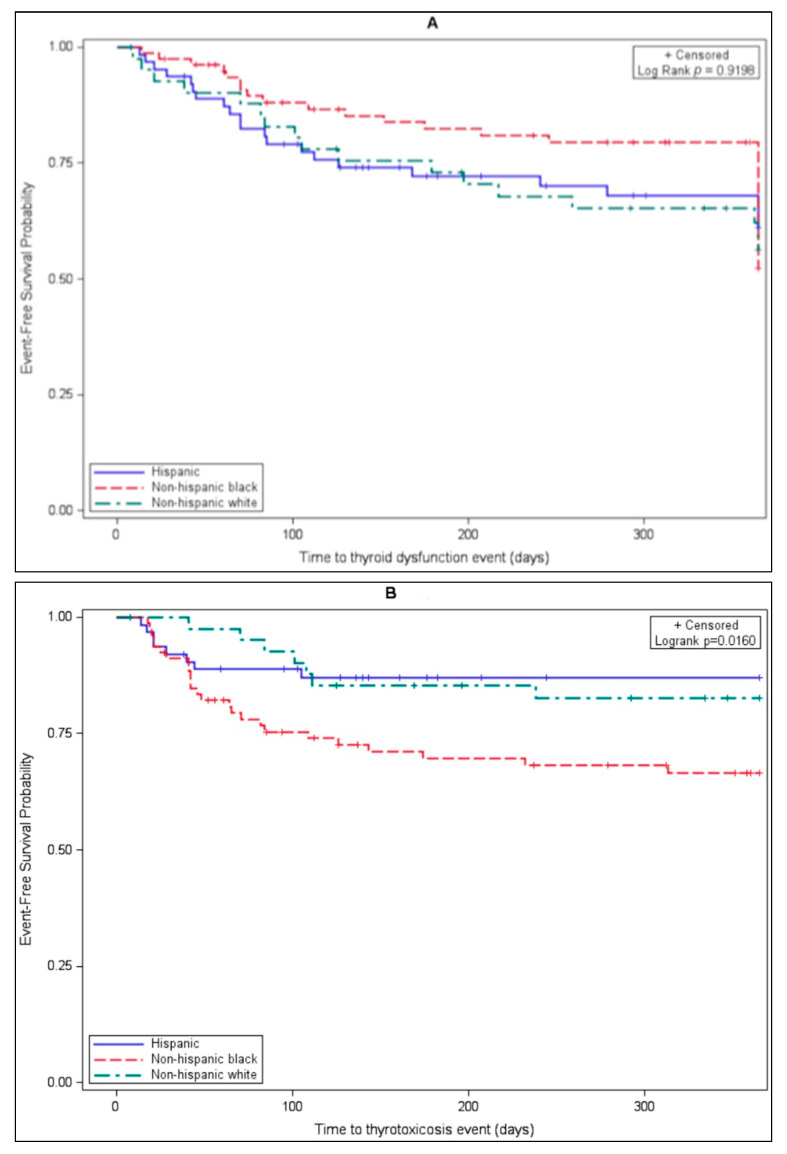
We sought to characterize thyroid dysfunction and its association with baseline clinical and demographic characteristics, as well as progression-free survival (PFS), in a multiethnic cohort of lung cancer patients treated with ICIs. A retrospective chart review of lung cancer patients receiving an anti-PD1 or PD-L1 agent was performed. Multivariate Cox proportional hazards were fitted to compare time to thyroid dysfunction among race subgroups controlling for age, gender, treatment type, and duration. Thyroid dysfunction was based on laboratory testing; clinical symptoms were not required. PFS at a 24-week landmark analysis point among patients with and without thyroid dysfunction was compared using a log-rank test. We identified 205 subjects that received ICIs, including 76 (37.1%) who developed thyroid dysfunction. Rates of thyroid dysfunction by one year occurred at similar frequencies among all races ( = 0.92). Gender and concurrent chemotherapy showed no significant association with thyroid dysfunction ( = 0.81 and = 0.67, respectively). Thyrotoxicosis occurred at higher rates in Black (25, 31.6%) subjects than in White (7, 16.7%) and Hispanic (8, 12.7%) subjects when employing the log-rank test ( = 0.016) and multivariate Cox regression (HR 0.48, = 0.09 for White and HR 0.36, = 0.01 for Hispanic compared to Black subjects). PFS was similar among subjects with and without thyroid dysfunction when applying the log-rank test ( = 0.353). Gender, concurrent treatment with chemotherapy, and PFS were not associated with thyroid dysfunction in patients receiving ICIs; however, Black race was a risk factor for thyrotoxicosis. The mechanisms underlying the role of race in the development of irAEs warrant further study.
我们试图在接受免疫检查点抑制剂(ICI)治疗的多民族肺癌患者队列中,明确甲状腺功能障碍及其与基线临床和人口统计学特征以及无进展生存期(PFS)的关联。对接受抗PD-1或PD-L1药物治疗的肺癌患者进行了回顾性病历审查。采用多变量Cox比例风险模型,在控制年龄、性别、治疗类型和疗程的情况下,比较不同种族亚组出现甲状腺功能障碍的时间。甲状腺功能障碍基于实验室检测结果,无需临床症状。使用对数秩检验比较有和无甲状腺功能障碍患者在24周标志性分析点的PFS。我们纳入了205例接受ICI治疗的受试者,其中76例(37.1%)出现了甲状腺功能障碍。所有种族在1年内出现甲状腺功能障碍的发生率相似(P = 0.92)。性别和同期化疗与甲状腺功能障碍均无显著关联(分别为P = 0.81和P = 0.67)。采用对数秩检验(P = 0.016)和多变量Cox回归分析(与黑人受试者相比,白人的风险比[HR]为0.48,P = 0.09;西班牙裔的HR为0.36,P = 0.01)时,黑人受试者(25例,31.6%)发生甲状腺毒症的比例高于白人(7例,16.7%)和西班牙裔(8例,12.7%)受试者。应用对数秩检验时,有和无甲状腺功能障碍受试者的PFS相似(P = 0.353)。接受ICI治疗的患者中,性别、同期化疗及PFS与甲状腺功能障碍均无关联;然而,黑人种族是发生甲状腺毒症的一个危险因素。种族在免疫相关不良反应发生中所起作用的潜在机制值得进一步研究。