Lamotte Guillaume, Sandroni Paola, Cutsforth-Gregory Jeremy K, Berini Sarah E, Benarroch Eduardo E, Shouman Kamal, Mauermann Michelle L, Anderson Jennifer, Low Phillip A, Singer Wolfgang, Coon Elizabeth A
Department of Neurology, Mayo Clinic, 200 1st Street SW, Rochester, MN, 55905, USA.
J Neurol. 2021 Oct;268(10):3852-3860. doi: 10.1007/s00415-021-10531-8. Epub 2021 Apr 3.
Ross syndrome is a rare disorder characterized by tonic pupils, hyporeflexia, and segmental anhidrosis. We sought to characterize the clinical presentation, associated autoimmune disorders, and autonomic profile in patients with Ross syndrome to further elucidate its pathophysiology.
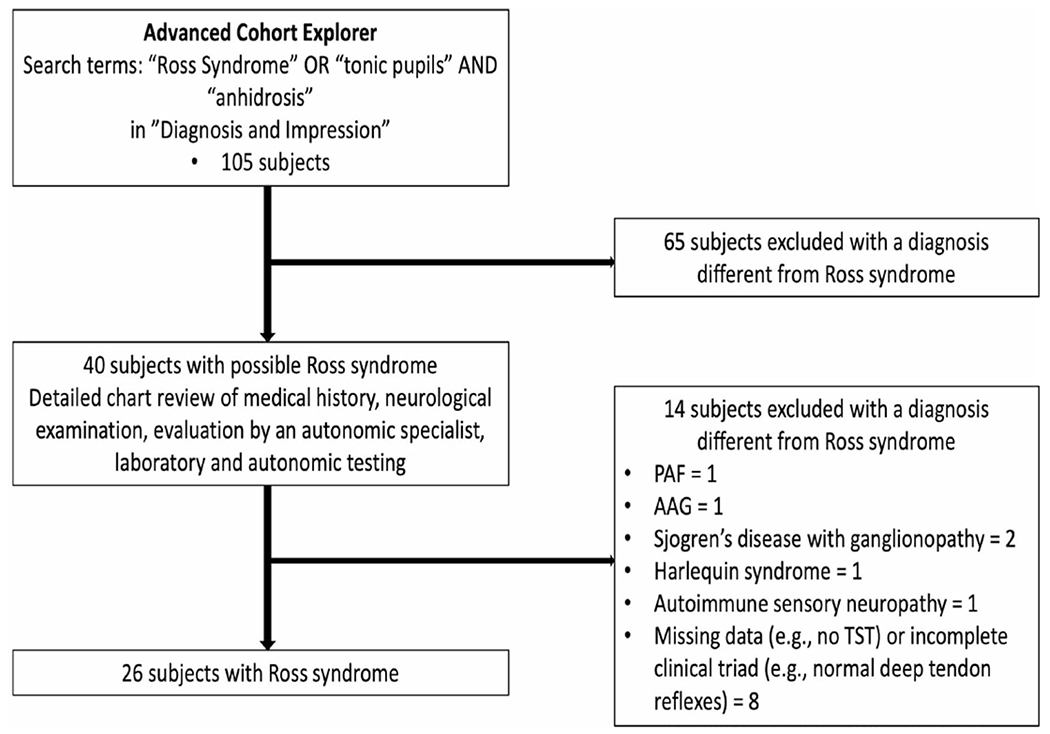
We performed a retrospective chart review of all patients who underwent a thermoregulatory sweat test (TST) between 1998 and 2020 and had confirmation of the diagnosis of Ross syndrome by an autonomic disorders specialist. Standardized autonomic reflex testing was reviewed when available.
Twenty-six patients with Ross syndrome were identified. The most common initial reported manifestation was an abnormal segmental sweating response in 16 patients (described as hyperhidrosis in 12 patients and anhidrosis in 4 patients) while a tonic pupil was the initial manifestation in 10 patients. Other commonly reported symptoms included fatigue, chronic cough, and increased urinary frequency. An associated autoimmune disorder was identified in one patient. Positive autoantibodies were found in a minority of patients often with unclear clinical significance. Distributions of anhidrosis encountered were segmental (n = 15), widespread (n = 7), and global (n = 4). Well-circumscribed small areas of preserved sweating within areas of anhidrosis were observed in the majority of patients (88.5%). Anhidrosis progressed slowly over time and sudomotor dysfunction was predominantly (post)ganglionic. Cardiovagal and adrenergic functions were preserved in most patients.
The pattern of autonomic dysfunction in Ross syndrome is suggestive of a limited autonomic ganglioneuropathy. Sudomotor impairment is prominent and should be the focus of symptomatic management; however, clinicians should be aware of symptoms beyond the classic triad.
罗斯综合征是一种罕见的疾病,其特征为瞳孔强直、反射减退和节段性无汗。我们试图描述罗斯综合征患者的临床表现、相关自身免疫性疾病和自主神经特征,以进一步阐明其病理生理学。
我们对1998年至2020年间接受体温调节汗液试验(TST)且经自主神经疾病专家确诊为罗斯综合征的所有患者进行了回顾性病历审查。如有可用,会审查标准化的自主神经反射测试。
共识别出26例罗斯综合征患者。最初报告的最常见表现是16例患者出现节段性出汗反应异常(12例描述为多汗,4例描述为无汗),而10例患者的最初表现为瞳孔强直。其他常见报告症状包括疲劳、慢性咳嗽和尿频增加。在1例患者中发现了相关的自身免疫性疾病。少数患者发现了阳性自身抗体,其临床意义通常不明确。无汗分布为节段性(n = 15)、广泛性(n = 7)和全身性(n = 4)。大多数患者(88.5%)在无汗区域内观察到界限清晰的小面积出汗保留区。无汗随时间缓慢进展,汗腺运动功能障碍主要为节后性。大多数患者的心血管迷走神经和肾上腺素能功能保留。
罗斯综合征的自主神经功能障碍模式提示为局限性自主神经节神经病。汗腺运动功能损害突出,应成为对症治疗的重点;然而临床医生应注意经典三联征以外的症状。