Department of Oncology, Hebei Petrochina Central Hospital, Heibei, Langfang, 065000, China.
World J Surg Oncol. 2021 Apr 6;19(1):99. doi: 10.1186/s12957-021-02203-8.
The American Society of Colon and Rectal Surgeons is suggesting laparoscopic surgeries for colorectal cancer. Conventional perioperative procedures like long preoperative fasting and bowel procedures are not useful and harmful to patients undergoing surgeries for colorectal cancer. The objectives of the study were to compare surgery outcomes, hospital stays, and survival of patients who received fast-track (laparoscopy/open) surgical procedure followed by chemotherapy against those who received conventional (laparoscopy/open) surgical procedure followed by chemotherapy for colorectal cancer.
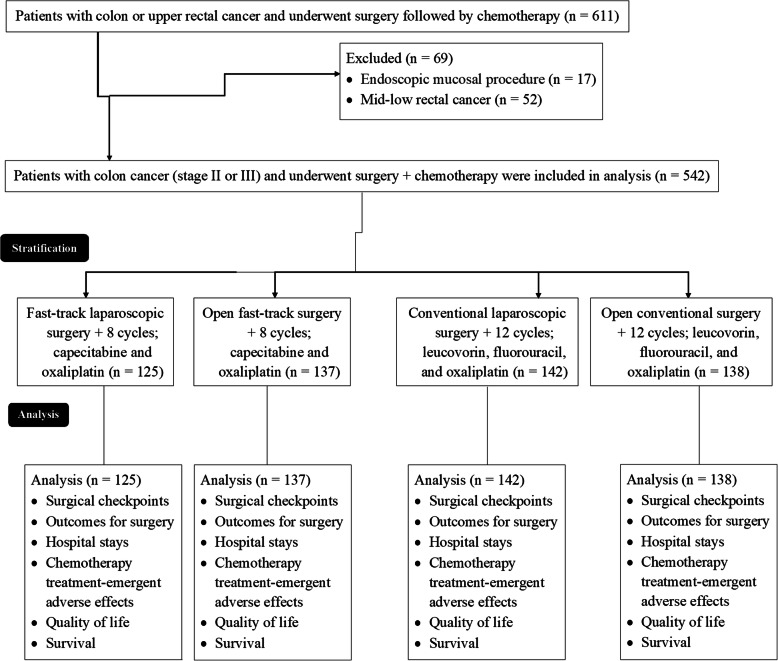
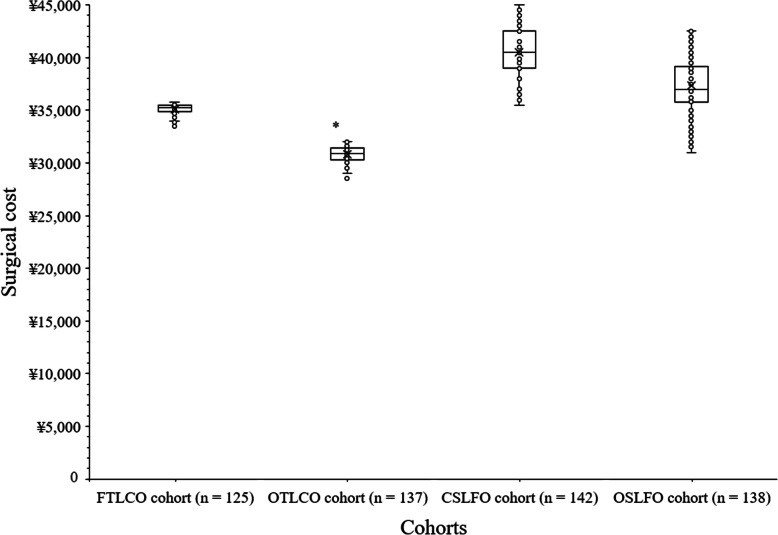
The study analyzes the outcomes of a total of 542 colorectal cancer (preoperative biopsies stage II or III) patients submitted to surgery and adjuvant chemotherapy. The study cohort is retrospectively subdivided in 4 groups submitted to open or laparoscopic resection with or without fast-track protocol appliance and two different chemotherapy regimens. Patients who ended up being TNM stage I have not received the adjuvant chemotherapy.
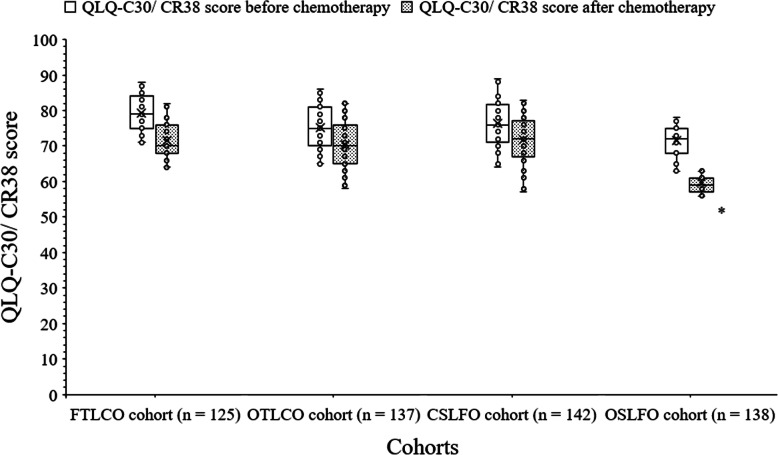
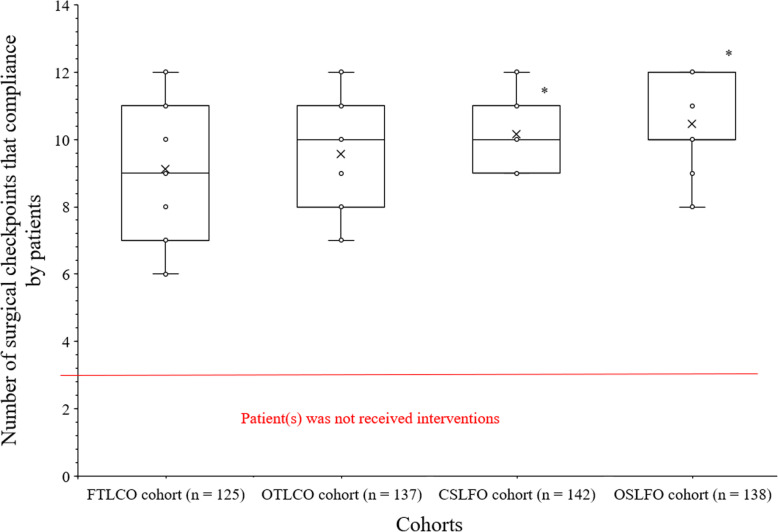
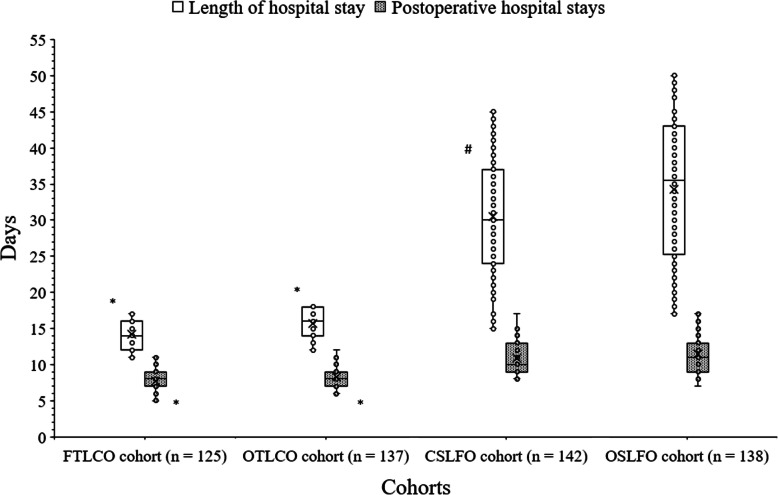
The fast-track surgical procedure had shorter total hospital stays and postoperative hospital stays than the conventional surgical procedures. Flatus resumption time, the time until first defecation, and intraoperative blood loss were shorter for the fast-track surgical procedures than the conventional surgical procedures. Those surgery outcomes were also shorter for the fast-track laparoscopy than the open fast-track. Resumption of a fluid diet and ambulation onset time were shorter for the fast-track surgical procedures than the conventional surgical procedures. The surgical checkpoints that were compliance by patient of fast-track surgeries were significantly fewer than those of the conventional surgeries. Clinically significant difference for QLQ-C30/CR38 score after chemotherapy was reported between patients who received open conventional surgeries and those patients who received fast-track laparoscopy (59.63 ± 2.26 score/patient vs. 71.67 ± 5.19 score/patient). There were no significant differences for the number of patients with any grade adverse effects (p = 0.431) or with grade 3-4 adverse effects (p = 0.858), and the disease-free and overall survival among cohorts.
The fast-track surgical procedure is effective and safe even in a multidisciplinary scenario as colorectal cancer treatment in which surgery is only a part of management.
III: Technical efficacy stage: 4.
美国结直肠外科医师学会建议对结直肠癌患者进行腹腔镜手术。传统的围手术期处理方法,如长时间的术前禁食和肠道准备,对接受结直肠癌手术的患者既无益又有害。本研究的目的是比较接受快速通道(腹腔镜/开放性)手术加化疗和接受常规(腹腔镜/开放性)手术加化疗的结直肠癌患者的手术结果、住院时间和生存率。
本研究分析了共 542 例结直肠癌(术前活检分期 II 期或 III 期)患者接受手术和辅助化疗的结果。该研究队列回顾性地分为 4 组,分别接受开放性或腹腔镜切除术,加或不加快速通道方案,并采用两种不同的化疗方案。最终分期为 TNM Ⅰ期的患者未接受辅助化疗。
快速通道手术的总住院时间和术后住院时间均短于常规手术。快速通道手术的肛门排气时间、首次排便时间和术中出血量均短于常规手术。快速通道腹腔镜手术的这些手术结果也短于开放快速通道。快速通道手术的恢复液体饮食和开始活动时间均短于常规手术。快速通道手术患者的手术检查点遵医行为明显少于常规手术患者。接受开放性常规手术的患者与接受快速通道腹腔镜手术的患者在化疗后 QLQ-C30/CR38 评分的临床显著差异(59.63 ± 2.26 分/患者比 71.67 ± 5.19 分/患者)。在任何等级不良事件的发生率(p = 0.431)或 3-4 级不良事件的发生率(p = 0.858),以及无病生存率和总生存率方面,各组之间均无显著差异。
即使在多学科治疗结直肠癌的情况下,快速通道手术也是有效和安全的,手术只是管理的一部分。
III:技术功效阶段:4。