JDRF/Wellcome Diabetes and Inflammation Laboratory, Wellcome Centre for Human Genetics, Nuffield Department of Medicine, University of Oxford, Oxford, UK.
Institute for Research in Genetics and Biomedicine (IRGB), Cagliari, Sardinia, Italy.
Diabetologia. 2021 Jun;64(6):1342-1347. doi: 10.1007/s00125-021-05428-0. Epub 2021 Apr 8.
AIMS/HYPOTHESIS: Given the potential shared aetiology between type 1 and type 2 diabetes, we aimed to identify any genetic regions associated with both diseases. For associations where there is a shared signal and the allele that increases risk to one disease also increases risk to the other, inference about shared aetiology could be made, with the potential to develop therapeutic strategies to treat or prevent both diseases simultaneously. Alternatively, if a genetic signal co-localises with divergent effect directions, it could provide valuable biological insight into how the association affects the two diseases differently.
Using publicly available type 2 diabetes summary statistics from a genome-wide association study (GWAS) meta-analysis of European ancestry individuals (74,124 cases and 824,006 controls) and type 1 diabetes GWAS summary statistics from a meta-analysis of studies on individuals from the UK and Sardinia (7467 cases and 10,218 controls), we identified all regions of 0.5 Mb that contained variants associated with both diseases (false discovery rate <0.01). In each region, we performed forward stepwise logistic regression to identify independent association signals, then examined co-localisation of each type 1 diabetes signal with each type 2 diabetes signal using coloc. Any association with a co-localisation posterior probability of ≥0.9 was considered a genuine shared association with both diseases.
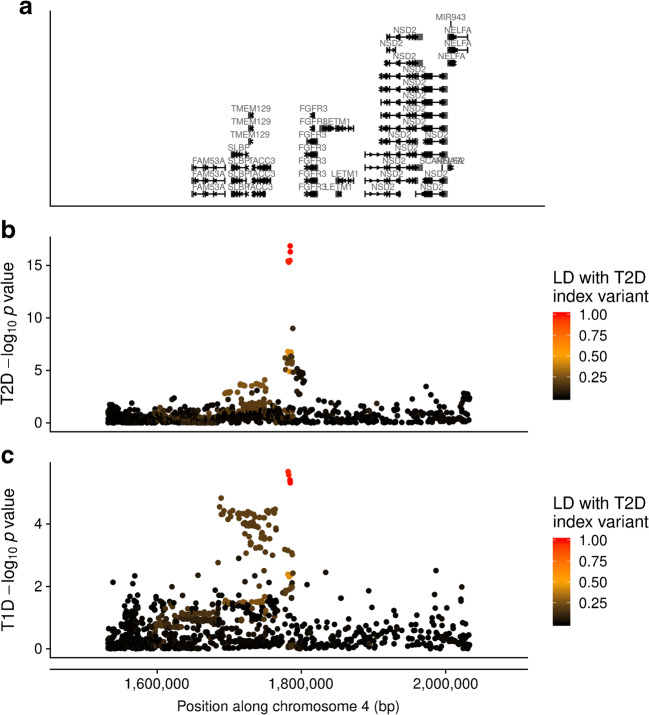
Of the 81 association signals from 42 genetic regions that showed association with both type 1 and type 2 diabetes, four association signals co-localised between both diseases (posterior probability ≥0.9): (1) chromosome 16q23.1, near CTRB1/BCAR1, which has been previously identified; (2) chromosome 11p15.5, near the INS gene; (3) chromosome 4p16.3, near TMEM129 and (4) chromosome 1p31.3, near PGM1. In each of these regions, the effect of genetic variants on type 1 diabetes was in the opposite direction to the effect on type 2 diabetes. Use of additional datasets also supported the previously identified co-localisation on chromosome 9p24.2, near the GLIS3 gene, in this case with a concordant direction of effect.
CONCLUSIONS/INTERPRETATION: Four of five association signals that co-localise between type 1 diabetes and type 2 diabetes are in opposite directions, suggesting a complex genetic relationship between the two diseases.
目的/假设:鉴于 1 型和 2 型糖尿病之间潜在的共同发病机制,我们旨在确定与这两种疾病相关的任何遗传区域。对于存在共同信号的关联,并且增加一种疾病风险的等位基因也增加另一种疾病的风险,则可以对共同发病机制进行推断,从而有可能开发出同时治疗或预防这两种疾病的治疗策略。或者,如果遗传信号与不同的效应方向共定位,则可以为两种疾病的关联如何产生不同影响提供有价值的生物学见解。
我们使用了公开的 2 型糖尿病全基因组关联研究(GWAS)荟萃分析的欧洲血统个体(74124 例病例和 824006 例对照)的汇总统计数据和来自英国和撒丁岛的研究的 1 型糖尿病 GWAS 汇总统计数据(7467 例病例和 10218 例对照),确定了包含与两种疾病相关的变异体的 0.5 Mb 区域(错误发现率<0.01)。在每个区域中,我们进行了向前逐步逻辑回归以确定独立的关联信号,然后使用 coloc 检查每个 1 型糖尿病信号与每个 2 型糖尿病信号的共定位。任何具有共同定位后验概率≥0.9 的关联均被认为与两种疾病具有真正的共同关联。
在与 1 型和 2 型糖尿病均相关的 42 个遗传区域的 81 个关联信号中,有 4 个关联信号在两种疾病之间共定位(后验概率≥0.9):(1)16 号染色体 16q23.1 附近的 CTRB1/BCAR1,先前已鉴定出;(2)11 号染色体 11p15.5 附近的 INS 基因;(3)4 号染色体 4p16.3 附近的 TMEM129 和(4)1 号染色体 1p31.3 附近的 PGM1。在这些区域中的每一个中,遗传变异对 1 型糖尿病的影响与对 2 型糖尿病的影响相反。使用其他数据集也支持了先前在 9 号染色体 9p24.2 附近 GLIS3 基因处的共定位,在这种情况下,效应方向一致。
结论/解释:在 1 型糖尿病和 2 型糖尿病之间共定位的 5 个关联信号中的 4 个信号处于相反的方向,表明这两种疾病之间存在复杂的遗传关系。