Alshahrani Mohammed S, Alatigue Rawan
Emergency and Critical Care Departments, King Fahd Hospital of the University, Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia.
Department of Emergency Medicine, King Fahd Specialist Hospital, Dammam, Kingdom of Saudi Arabia.
Open Access Emerg Med. 2021 Mar 31;13:143-150. doi: 10.2147/OAEM.S298315. eCollection 2021.
Septic shock still carries a high mortality rate despite all advances in emergency and critical care practices. Early interventions have been proven in many aspects to improve outcome. However, early administration of vasopressors namely norepinephrine in septic shock is still controversial.
To identify the association between early norepinephrine administration and mortality in septic shock patients.
A retrospective review of a prospectively collected ICU data for septic shock patients in medical and surgical intensive care units for one year period was carried out. Case definition was based on sepsis 3 definitions. Data included patients' characteristics of demographics, admission diagnosis, APACHE II score, physiological data (including vital signs and laboratory values). The primary outcome was 28 days of mortality.
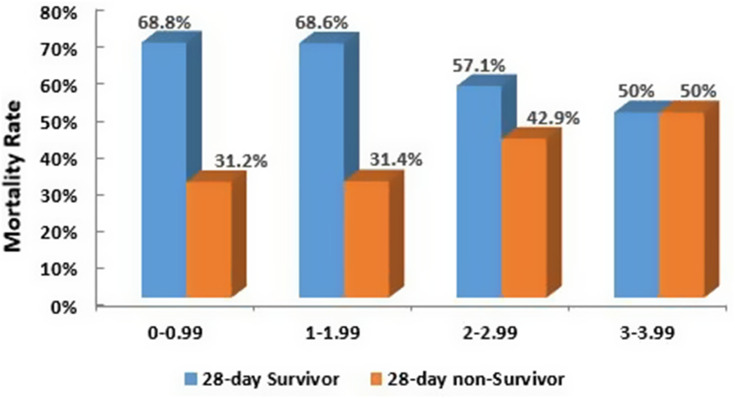
A total of 243 patients identified during the study period, 132 (54.3%) were male. The mean age was found to be 58.9 ± 20.3. The overall rate of 28 days mortality was 87 (47.5%). Norepinephrine was started for 68.9% of the patients in ICU, the rest were started in the emergency department. The highest survival rates were among patients who received norepinephrine within first hour (58.1%) and second (51.5%). A binary logistic regression analysis has been performed to adjust for possible confounders. It was revealed that being intubated and mechanically ventilated or having higher APACHE II score were strongly associated with non-survival rates (OR=7.049, p-0.002), (OR=1.124, p-<0.001) respectively.
Our results showed that septic shock patients who had early administration of norepinephrine had a higher survival rate. Intubation and invasive ventilation and higher APACHE II score associated with higher none survival rate.
尽管急诊和重症监护实践取得了诸多进展,但感染性休克的死亡率仍然很高。早期干预已在许多方面被证明可改善预后。然而,在感染性休克中早期使用血管升压药,即去甲肾上腺素,仍存在争议。
确定感染性休克患者早期使用去甲肾上腺素与死亡率之间的关联。
对内科和外科重症监护病房前瞻性收集的感染性休克患者的ICU数据进行了为期一年的回顾性分析。病例定义基于脓毒症3的定义。数据包括患者的人口统计学特征、入院诊断、急性生理与慢性健康状况评分系统(APACHE II)评分、生理数据(包括生命体征和实验室值)。主要结局是28天死亡率。
在研究期间共确定了243例患者,其中132例(54.3%)为男性。平均年龄为58.9±20.3岁。28天死亡率的总体发生率为87例(47.5%)。68.9%的患者在ICU开始使用去甲肾上腺素,其余患者在急诊科开始使用。在第一小时内接受去甲肾上腺素治疗的患者生存率最高(58.1%),其次是第二小时(51.5%)。进行了二元逻辑回归分析以调整可能的混杂因素。结果显示,插管并机械通气或APACHE II评分较高与死亡率密切相关(比值比分别为7.049,p = 0.002),(比值比为1.124,p < 0.001)。
我们的结果表明,早期使用去甲肾上腺素的感染性休克患者生存率较高。插管和有创通气以及较高的APACHE II评分与较高的死亡率相关。