Wu Chaoqun, Zhang Danwei, Bai Xueke, Zhou Tiannan, Wang Yongfei, Lin Zhenqiu, He Guangda, Li Xi
National Clinical Research Center of Cardiovascular Diseases, NHC Key Laboratory of Clinical Research for Cardiovascular Medications, State Key Laboratory of Cardiovascular Disease, Fuwai Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, National Center for Cardiovascular Diseases, Beijing, China.
Center for Outcomes Research and Evaluation, Yale-New Haven Health System, New Haven, Connecticut, USA.
BMJ Open. 2021 Apr 9;11(4):e045053. doi: 10.1136/bmjopen-2020-045053.
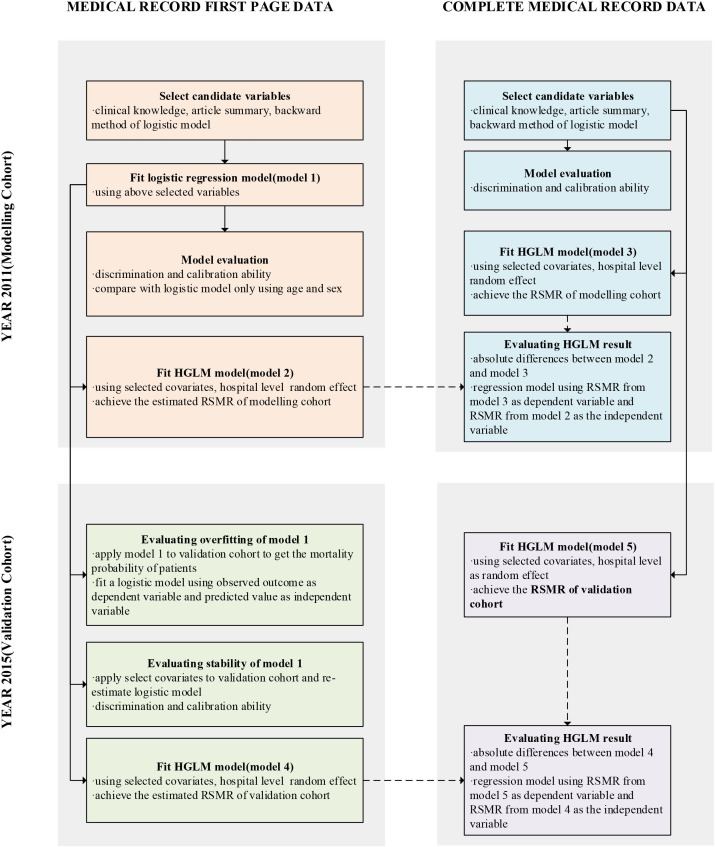
To develop a model of in-hospital mortality using medical record front page (MRFP) data and assess its validity in case-mix standardisation by comparison with a model developed using the complete medical record data.
A nationally representative retrospective study.
Representative hospitals in China, covering 161 hospitals in modelling cohort and 156 hospitals in validation cohort.
Representative patients admitted for acute myocardial infarction. 8370 patients in modelling cohort and 9704 patients in validation cohort.
In-hospital mortality, which was defined explicitly as death that occurred during hospitalisation, and the hospital-level risk standardised mortality rate (RSMR).
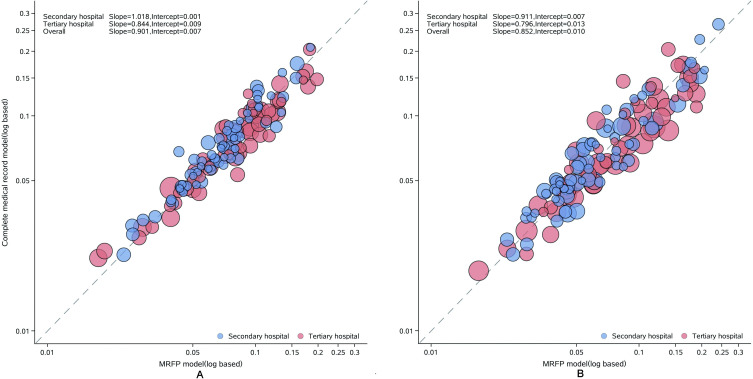
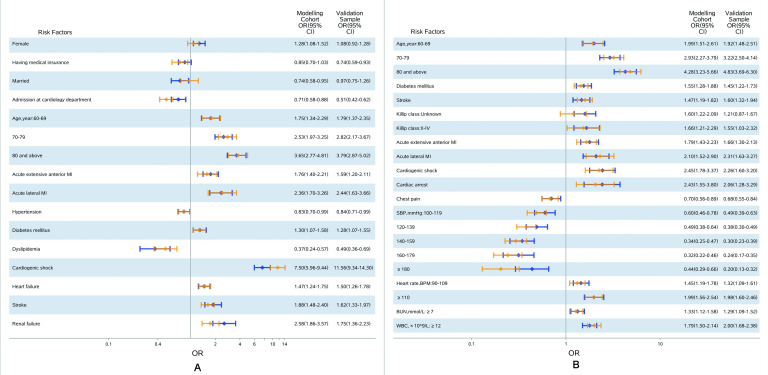
A total of 14 variables were included in the model predicting in-hospital mortality based on MRFP data, with the area under receiver operating characteristic curve of 0.78 among modelling cohort and 0.79 among validation cohort. The median of absolute difference between the hospital RSMR predicted by hierarchical generalised linear models established based on MRFP data and complete medical record data, which was built as 'reference model', was 0.08% (10th and 90th percentiles: -1.8% and 1.6%). In the regression model comparing the RSMR between two models, the slope and intercept of the regression equation is 0.90 and 0.007 in modelling cohort, while 0.85 and 0.010 in validation cohort, which indicated that the evaluation capability from two models were very similar.
The models based on MRFP data showed good discrimination and calibration capability, as well as similar risk prediction effect in comparison with the model based on complete medical record data, which proved that MRFP data could be suitable for risk adjustment in hospital performance measurement.
利用病历首页(MRFP)数据建立院内死亡率模型,并通过与使用完整病历数据建立的模型进行比较,评估其在病例组合标准化中的有效性。
一项具有全国代表性的回顾性研究。
中国的代表性医院,建模队列中有161家医院,验证队列中有156家医院。
因急性心肌梗死入院的代表性患者。建模队列中有8370例患者,验证队列中有9704例患者。
院内死亡率,明确定义为住院期间发生的死亡,以及医院层面的风险标准化死亡率(RSMR)。
基于MRFP数据预测院内死亡率的模型共纳入14个变量,建模队列中受试者操作特征曲线下面积为0.78,验证队列中为0.79。基于MRFP数据建立的分层广义线性模型预测的医院RSMR与作为“参考模型”构建的完整病历数据之间的绝对差异中位数为0.08%(第10和第90百分位数:-1.8%和1.6%)。在比较两个模型RSMR的回归模型中,建模队列中回归方程的斜率和截距分别为0.90和0.007,验证队列中为0.85和0.010,这表明两个模型的评估能力非常相似。
基于MRFP数据的模型显示出良好的区分度和校准能力,与基于完整病历数据的模型相比,风险预测效果相似,这证明MRFP数据可适用于医院绩效评估中的风险调整。