Kaku Ryosuke, Yoden Makoto, Shiratori Takuya, Hayashi Kazuki, Okamoto Keigo, Oshio Yasuhiko, Nakano Yasutaka, Hanaoka Jun
Division of General Thoracic Surgery, Department of Surgery, Shiga University of Medical Science, Shiga, Japan.
Division of Respiratory Medicine, Department of Internal Medicine, Shiga University of Medical Science, Shiga, Japan.
J Thorac Dis. 2021 Mar;13(3):1347-1357. doi: 10.21037/jtd-20-3090.
Respiratory function declines after lung resection. However, perioperative changes in respiratory impedance and their clinical significance are unclear. The forced oscillation technique can measure respiratory impedance during quiet breathing and possibly early after surgery. We investigated respiratory impedance changes before and after lung lobectomy and examined the correlation of impedance with clinical factors.
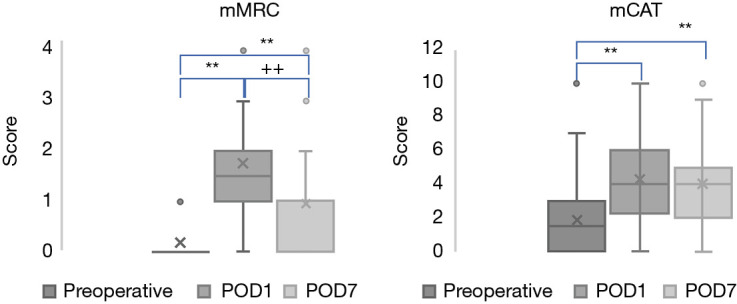
We prospectively included patients who underwent lobectomy between February 2018 and March 2020 and measured respiratory impedance by forced oscillation preoperatively and postoperative days 1 and 7. We statistically analyzed changes in perioperative forced oscillation measurements and their correlation with clinical factors, including subjective symptoms. The modified British Medical Research Council scale and the chronic obstructive pulmonary disease (COPD) assessment test were used for scoring subjective symptoms.
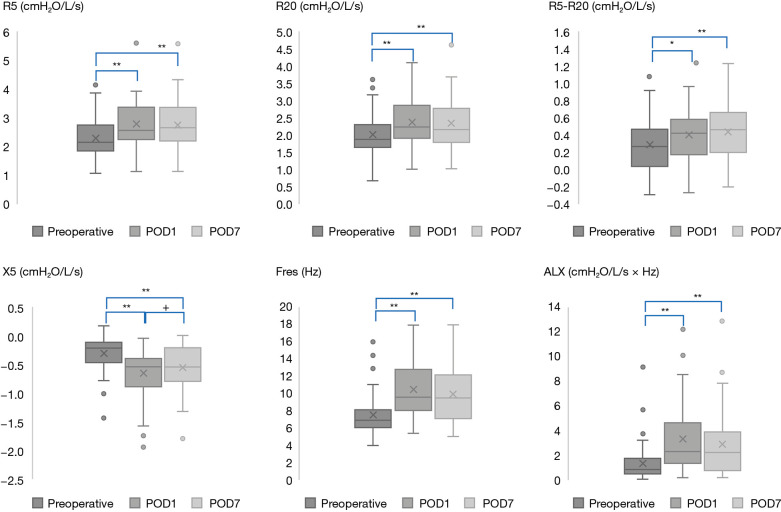
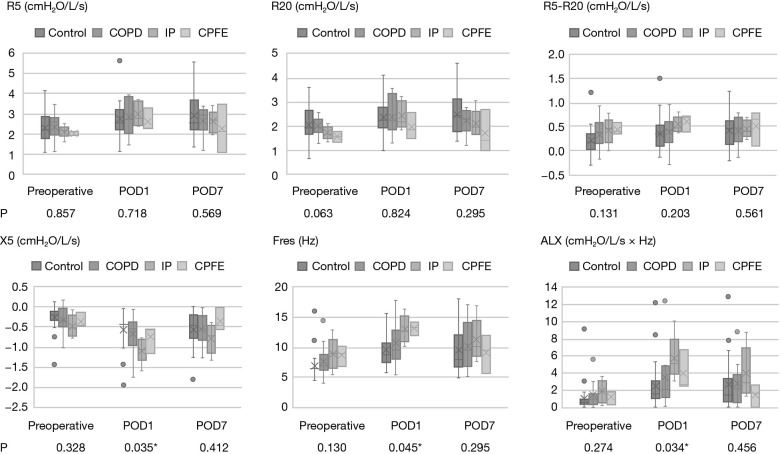
Forty-four subjects were included, in whom respiratory impedance could be measured from postoperative day 1. The respective mean values for forced oscillation measurements preoperatively and at postoperative days 1 and 7 were as follows: respiratory resistance, 5 Hz: 2.28, 2.77, and 2.75; respiratory resistance, 20 Hz: 2.00, 2.36, and 2.32; difference in respiratory resistance at 5 and 20 Hz: 0.28, 0.40, and 0.43; respiratory reactance, 5 Hz: -0.31, -0.65, and -0.56; resonant frequency: 7.45, 10.41, and 9.81; and low-frequency reactance area: 1.33, 3.27, and 2.84. These changes were statistically significant (P<0.01). Besides the difference in respiratory resistance at 5 and 20 Hz, all other measurements on postoperative day 7 were relatively weakly correlated with the modified Medical Research Council scale score at this time point (all P<0.05). Respiratory complications correlated with the respiratory resistance difference, respiratory reactance, and resonant frequency on day 7 (R =0.415, -0.421, and 0.441), while the latter also correlated with postoperative hypoxemia on day 1 (R =0.433).
Respiratory impedance was measurable even early after surgery and significantly changed postoperatively. As the sample size was small and appeared to be biased, assessing respiratory impedance and clinical factors in detail was difficult. Since respiratory impedance is suggested to be associated with clinical factors that affect the postoperative course, it is necessary to accumulate cases and observe them over longer periods.
肺切除术后呼吸功能会下降。然而,围手术期呼吸阻抗的变化及其临床意义尚不清楚。强迫振荡技术可在静息呼吸期间以及术后早期测量呼吸阻抗。我们研究了肺叶切除术前、后的呼吸阻抗变化,并探讨了阻抗与临床因素之间的相关性。
我们前瞻性纳入了2018年2月至2020年3月期间接受肺叶切除术的患者,并在术前、术后第1天和第7天通过强迫振荡测量呼吸阻抗。我们对围手术期强迫振荡测量值的变化及其与包括主观症状在内的临床因素之间的相关性进行了统计学分析。采用改良的英国医学研究委员会量表和慢性阻塞性肺疾病(COPD)评估测试对主观症状进行评分。
纳入44例受试者,术后第1天可测量呼吸阻抗。术前、术后第1天和第7天强迫振荡测量的各自平均值如下:呼吸阻力,5Hz:2.28、2.77和2.75;呼吸阻力,20Hz:2.00、2.36和2.32;5Hz和20Hz呼吸阻力差值:0.28、0.40和0.43;呼吸电抗,5Hz:-0.31、-0.65和-0.56;共振频率:7.45、10.41和9.81;低频电抗面积:1.33、3.27和2.84。这些变化具有统计学意义(P<0.01)。除了5Hz和20Hz呼吸阻力差值外,术后第7天的所有其他测量值与此时的改良医学研究委员会量表评分的相关性相对较弱(均P<0.05)。呼吸并发症与第7天的呼吸阻力差值、呼吸电抗和共振频率相关(R =0.415、-0.421和0.441),而后者也与术后第1天的低氧血症相关(R =0.433)。
即使在术后早期也可测量呼吸阻抗,且术后呼吸阻抗有显著变化。由于样本量小且似乎存在偏倚,难以详细评估呼吸阻抗与临床因素。鉴于呼吸阻抗被认为与影响术后病程的临床因素相关,有必要积累病例并进行更长时间的观察。