Adult Bone Marrow Transplant (BMT) Service, Memorial Sloan Kettering Cancer Center, New York, NY.
Department of Internal Medicine, Weill Cornell School of Medicine, New York, NY; and.
Blood Adv. 2021 Apr 13;5(7):2003-2011. doi: 10.1182/bloodadvances.2020002701.
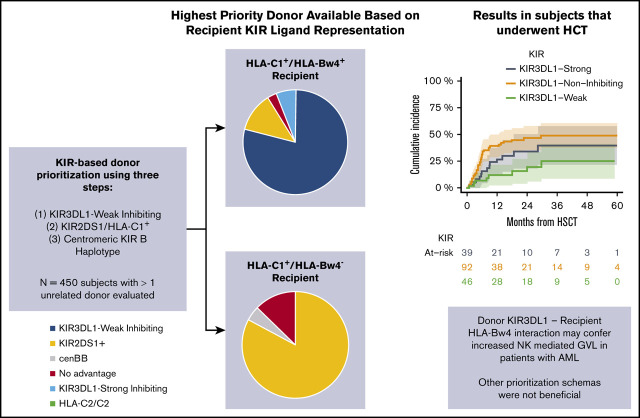
Donor KIR and recipient HLA combinations that minimize inhibition and favor activation of the NK repertoire are associated with improved outcomes after allogeneic hematopoietic cell transplantation (HCT) in patients with myeloid neoplasia. We prospectively evaluated a weighted donor ranking algorithm designed to prioritize HLA-compatible unrelated donors (URDs) with weak inhibitory KIR3DL1/HLA-Bw4 interaction, followed by donors with nontolerized activating KIR2DS1, and finally those with KIR centromeric B haplotype. During donor evaluation, we performed KIR genotyping and ranked 2079 URDs for 527 subjects with myelodysplastic syndrome (MDS) or acute myelogenous leukemia (AML). Among all patients, 394 (75%) had at least 1 KIR-advantageous donor, and 263 (50%) underwent HCT. In patients with AML, KIR3DL1 weak inhibition provided protection from relapse. Compared with KIR3DL1-Weak Inhibiting donors, KIR3DL1-Noninteracting donors were associated with increased risk of relapse (HR, 2.97; 95% CI, 1.33-6.64; P = .008) and inferior event-free survival (EFS; HR, 2.14; 95% CI, 1.16-3.95; P = .015). KIR3DL1-Strong Inhibiting donors were associated with HR, 1.65 (95% CI, 0.66-4.08; P = .25) for AML relapse and HR, 1.6 (95% CI, 0.81-3.17; P = .1) for EFS when compared with the use of KIR3DL1-weak inhibiting donors. Donor KIR2DS1/HLA-C1 status and centromeric KIR haplotype-B content were not associated with decreased risk of AML relapse. There was no benefit to KIR-based donor selection in patients with MDS. This study demonstrates that donor KIR typing is feasible, and prioritization of donors with certain KIR3DL1 genotypes may confer a protection from relapse after HCT in patients with AML.
供体 KIR 和受体 HLA 组合,最大限度地减少抑制作用并有利于 NK 库的激活,与骨髓增生性肿瘤患者异基因造血细胞移植 (HCT) 后的改善结果相关。我们前瞻性地评估了一种加权供体排序算法,旨在优先考虑与 HLA 相容的非亲缘供体 (URD),这些供体具有较弱的抑制性 KIR3DL1/HLA-Bw4 相互作用,其次是对激活性 KIR2DS1 未耐受的供体,最后是具有 KIR 着丝粒 B 单倍型的供体。在供体评估期间,我们对 2079 名 URD 进行了 KIR 基因分型,并对 527 名骨髓增生异常综合征 (MDS) 或急性髓系白血病 (AML) 患者进行了排名。在所有患者中,394 名 (75%) 至少有 1 名 KIR 有利供体,其中 263 名 (50%) 接受了 HCT。在 AML 患者中,KIR3DL1 弱抑制作用可防止复发。与 KIR3DL1 弱抑制供体相比,KIR3DL1 非相互作用供体与复发风险增加相关 (HR, 2.97;95%CI, 1.33-6.64;P =.008) 和无事件生存 (EFS) 降低 (HR, 2.14;95%CI, 1.16-3.95;P =.015)。与使用 KIR3DL1 弱抑制供体相比,KIR3DL1 强抑制供体与 AML 复发的 HR 为 1.65 (95%CI, 0.66-4.08;P =.25),与 EFS 的 HR 为 1.6 (95%CI, 0.81-3.17;P =.1)。供体 KIR2DS1/HLA-C1 状态和着丝粒 KIR 单倍型-B 含量与 AML 复发风险降低无关。在 MDS 患者中,基于 KIR 的供体选择没有获益。这项研究表明,供体 KIR 分型是可行的,优先选择某些 KIR3DL1 基因型的供体可能会在 AML 患者的 HCT 后防止复发。