Sugawara Toshitaka, Ban Daisuke, Nishino Jo, Watanabe Shuichi, Maekawa Aya, Ishikawa Yoshiya, Akahoshi Keiichi, Ogawa Kosuke, Ono Hiroaki, Kudo Atsushi, Tanaka Shinji, Tanabe Minoru
Department of Hepatobiliary and Pancreatic Surgery, Graduate School of Medicine, Tokyo Medical and Dental University, Tokyo, Japan.
Division of Bioinformatics, Research Institute, National Cancer Center Japan, Tokyo, Japan.
PLoS One. 2021 Apr 12;16(4):e0249885. doi: 10.1371/journal.pone.0249885. eCollection 2021.
Even after curative resection, pancreatic ductal adenocarcinoma (PDAC) patients suffer a high rate of recurrence. There is an unmet need to predict which patients will experience early recurrence after resection in order to adjust treatment strategies.
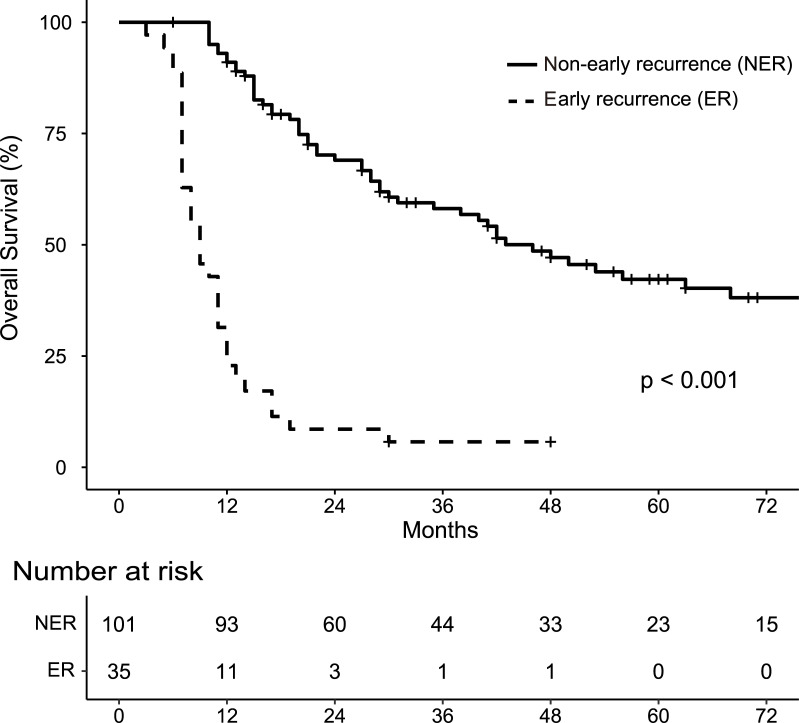
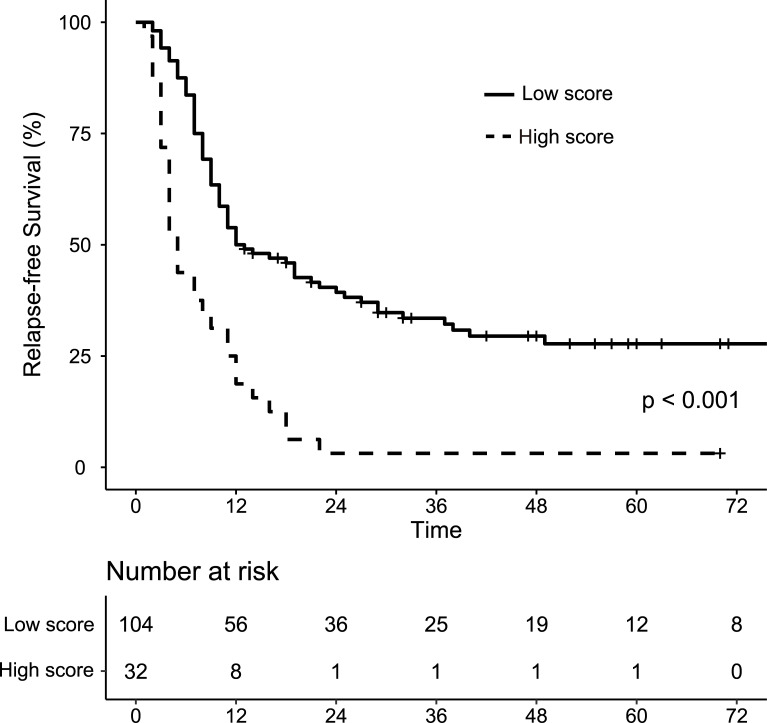
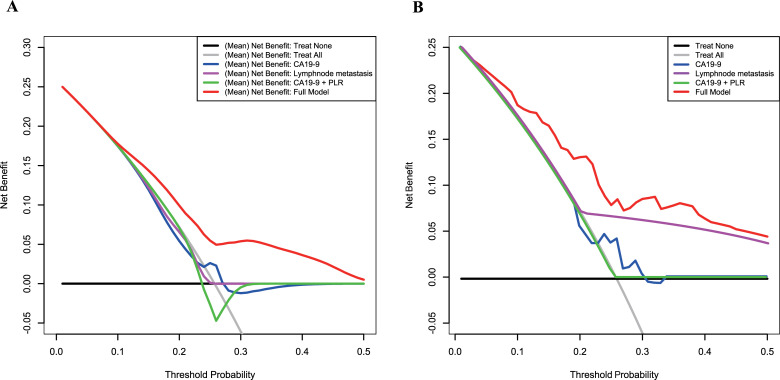
Data of patients with resectable PDAC undergoing surgical resection between January 2005 and September 2018 were reviewed to stratify for early recurrence defined as occurring within 6 months of resection. Preoperative data including demographics, tumor markers, blood immune-inflammatory factors and clinicopathological data were examined. We employed Elastic Net, a sparse modeling method, to construct models predicting early recurrence using these multiple preoperative factors. As a result, seven preoperative factors were selected: age, duke pancreatic monoclonal antigen type 2 value, neutrophil:lymphocyte ratio, systemic immune-inflammation index, tumor size, lymph node metastasis and is peripancreatic invasion. Repeated 10-fold cross-validations were performed, and area under the receiver operating characteristic curve (AUC) and decision curve analysis were used to evaluate the usefulness of the models.
A total of 136 patients was included in the final analysis, of which 35 (34%) experienced early recurrence. Using Elastic Net, we found that 7 of 14 preoperative factors were useful for the predictive model. The mean AUC of all models constructed in the repeated validation was superior to the standard marker CA 19-9 (0.718 vs 0.657), whereas the AUC of the model constructed from the entire patient cohort was 0.767. Decision curve analysis showed that the models had a higher mean net benefit across the majority of the range of reasonable threshold probabilities.
A model using multiple preoperative factors can improve prediction of early resectable PDAC recurrence.
即使进行了根治性切除,胰腺导管腺癌(PDAC)患者的复发率仍很高。为了调整治疗策略,预测哪些患者在切除后会早期复发的需求尚未得到满足。
回顾了2005年1月至2018年9月期间接受手术切除的可切除性PDAC患者的数据,以对定义为切除后6个月内发生的早期复发进行分层。检查了术前数据,包括人口统计学、肿瘤标志物、血液免疫炎症因子和临床病理数据。我们采用弹性网络(一种稀疏建模方法),使用这些多个术前因素构建预测早期复发的模型。结果,选择了七个术前因素:年龄、杜克胰腺单克隆抗原2型值、中性粒细胞与淋巴细胞比率、全身免疫炎症指数、肿瘤大小、淋巴结转移和是否存在胰周侵犯。进行了重复的10倍交叉验证,并使用受试者操作特征曲线下面积(AUC)和决策曲线分析来评估模型的有效性。
最终分析共纳入136例患者,其中35例(34%)发生早期复发。使用弹性网络,我们发现14个术前因素中的7个对预测模型有用。在重复验证中构建的所有模型的平均AUC优于标准标志物CA 19-9(0.718对0.657),而从整个患者队列构建的模型的AUC为0.767。决策曲线分析表明,在大多数合理阈值概率范围内,模型具有更高的平均净效益。
使用多个术前因素的模型可以改善对可切除性PDAC早期复发的预测。