Cartwright Bruce, Bruce Hannah M, Kershaw Geoffrey, Cai Nancy, Othman Jad, Gattas David, Robson Jacqueline L, Hayes Sarah, Alicajic Hayden, Hines Anna, Whyte Alice, Chaikittisilpa Nophanan, Southwood Timothy James, Forrest Paul, Totaro Richard J, Bannon Paul G, Dunkley Scott, Chen Vivien M, Dennis Mark
Sydney Medical School, University of Sydney, Sydney, Australia.
Department of Anaesthetics, Royal Prince Alfred Hospital, Sydney, Australia.
Sci Rep. 2021 Apr 12;11(1):7975. doi: 10.1038/s41598-021-87026-z.
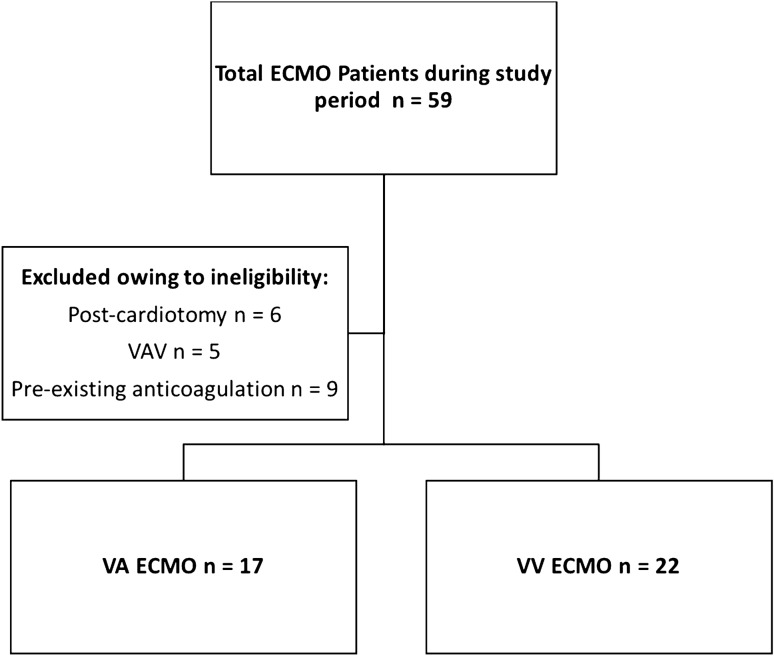
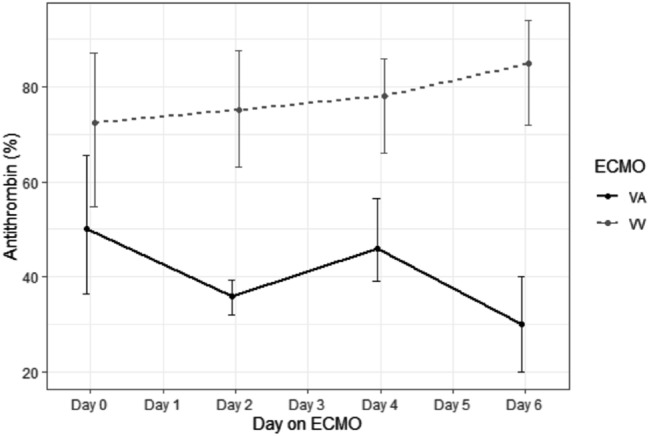
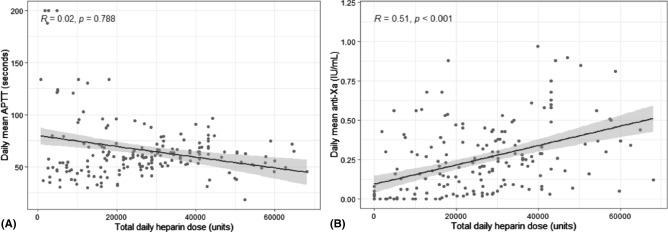
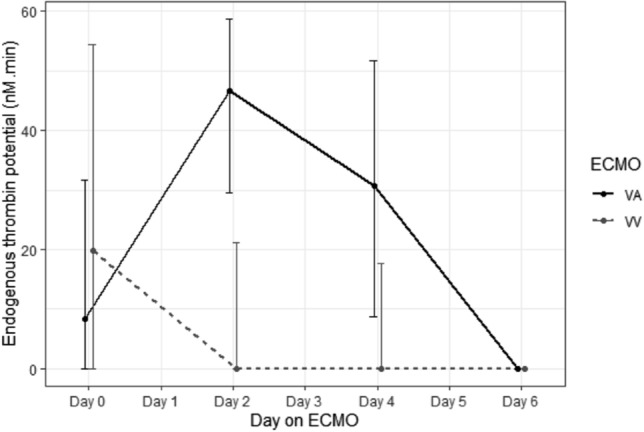
Extracorporeal membrane oxygenation (ECMO) support has a high incidence of both bleeding and thrombotic complications. Despite clear differences in patient characteristics and pathologies between veno-venous (VV) and veno-arterial (VA) ECMO support, anticoagulation practices are often the same across modalities. Moreover, there is very little data on their respective coagulation profiles and comparisons of thrombin generation in these patients. This study compares the coagulation profile and thrombin generation between patients supported with either VV and VA ECMO. A prospective cohort study of patients undergoing VA and VV ECMO at an Intensive care department of a university hospital and ECMO referral centre. In addition to routine coagulation testing and heparin monitoring per unit protocol, thromboelastography (TEG), multiplate aggregometry (MEA), calibrated automated thrombinography (CAT) and von-Willebrand's activity (antigen and activity ratio) were sampled second-daily for 1 week, then weekly thereafter. VA patients had significantly lower platelets counts, fibrinogen, anti-thrombin and clot strength with higher d-dimer levels than VV patients, consistent with a more pronounced consumptive coagulopathy. Thrombin generation was higher in VA than VV patients, and the heparin dose required to suppress thrombin generation was lower in VA patients. There were no significant differences in total bleeding or thrombotic event rates between VV and VA patients when adjusted for days on extracorporeal support. VA patients received a lower median daily heparin dose 8500 IU [IQR 2500-24000] versus VV 28,800 IU [IQR 17,300-40,800.00]; < 0.001. Twenty-eight patients (72%) survived to hospital discharge; comprising 53% of VA patients and 77% of VV patients. Significant differences between the coagulation profiles of VA and VV patients exist, and anticoagulation strategies for patients of these modalities should be different. Further research into the development of tailored anticoagulation strategies that include the mode of ECMO support need to be completed.
体外膜肺氧合(ECMO)支持治疗中出血和血栓形成并发症的发生率很高。尽管静脉-静脉(VV)和静脉-动脉(VA)ECMO支持治疗的患者特征和病理情况存在明显差异,但不同模式下的抗凝措施通常相同。此外,关于这些患者各自的凝血谱以及凝血酶生成比较的数据非常少。本研究比较了接受VV和VA ECMO支持治疗患者的凝血谱和凝血酶生成情况。这是一项在大学医院重症监护病房和ECMO转诊中心对接受VA和VV ECMO治疗的患者进行的前瞻性队列研究。除了按照单位方案进行常规凝血检测和肝素监测外,在第1周每天采样一次血栓弹力图(TEG)、多电极血小板聚集检测(MEA)、校准自动凝血酶生成检测(CAT)和血管性血友病因子活性(抗原和活性比值),之后每周采样一次。与VV患者相比,VA患者的血小板计数、纤维蛋白原、抗凝血酶和凝血强度显著降低,而D-二聚体水平更高,这与更明显的消耗性凝血病一致。VA患者的凝血酶生成高于VV患者,且VA患者抑制凝血酶生成所需的肝素剂量更低。在校正体外支持天数后,VV和VA患者的总出血或血栓形成事件发生率没有显著差异。VA患者的每日肝素剂量中位数较低,为8500国际单位[四分位间距2500 - 24000],而VV患者为28800国际单位[四分位间距17300 - 40800.00];P<0.001。28例患者(72%)存活至出院;其中VA患者占53%,VV患者占77%。VA和VV患者的凝血谱存在显著差异,针对这些模式患者的抗凝策略应该不同。需要完成进一步研究以制定包括ECMO支持模式的量身定制的抗凝策略。