Lee Jung Su, Lee Jeong Hoon, Kim Jinyoung, Na Hee Kyong, Ahn Ji Yong, Jung Kee Wook, Kim Do Hoon, Choi Kee Don, Song Ho June, Lee Gin Hyug, Jung Hwoon Yong
Division of Gastroenterology, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
Division of Gastroenterology, Department of Internal Medicine, Ilsan Paik Hospital, Inje University College of Medicine, Goyang, Korea.
J Korean Med Sci. 2021 Apr 12;36(14):e88. doi: 10.3346/jkms.2021.36.e88.
Endoscopic surveillance after total gastrectomy (TG) for gastric cancer is routinely performed to detect tumor recurrence and postoperative adverse events. However, the reports on the clinical benefits of endoscopic surveillance are ambiguous. We investigated the clinical benefit of endoscopic surveillance after TG for gastric cancer.
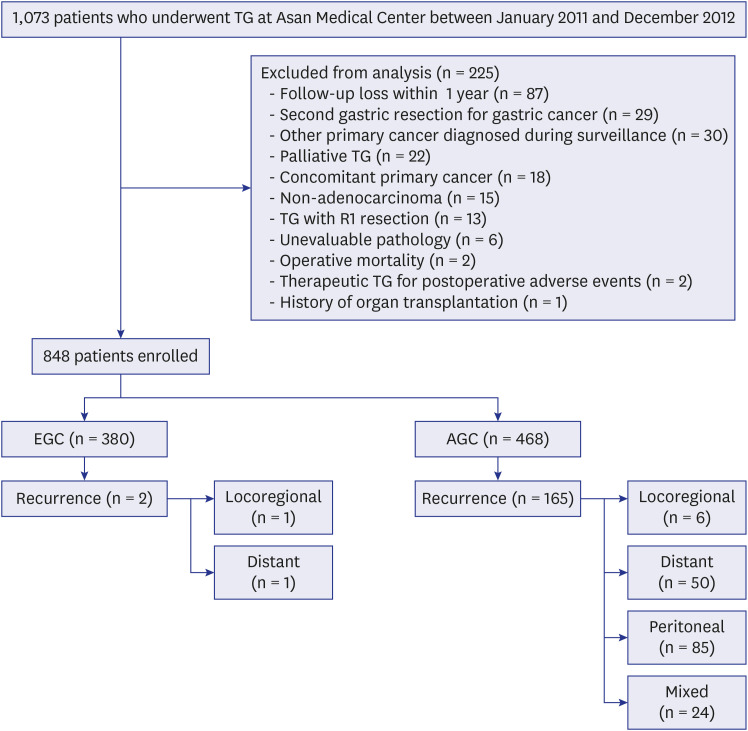
We analyzed 848 patients who underwent TG with R0 resection for gastric cancer between 2011 and 2012 (380 early gastric cancer and 468 advanced gastric cancer) and underwent regular postoperative surveillance with endoscopy and abdominopelvic computed tomography (CT) with contrast.
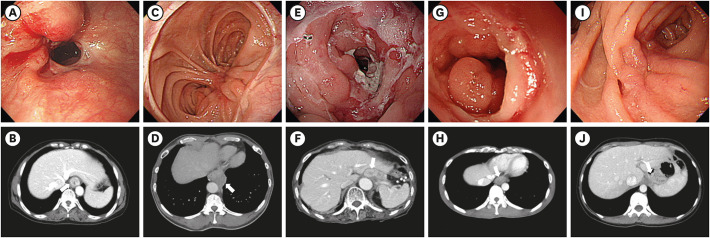
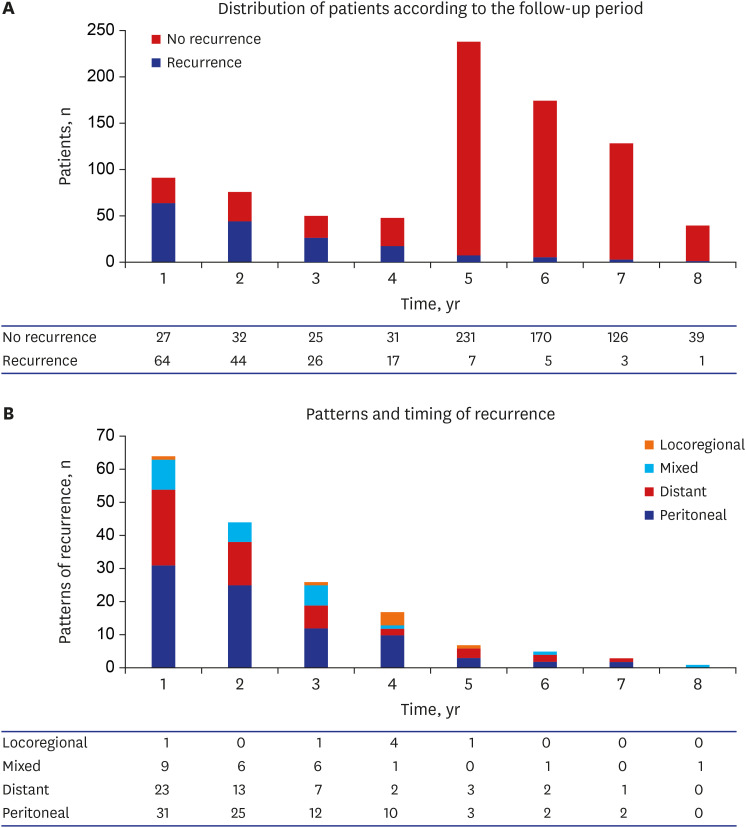
Median follow-up periods were 58 months for both endoscopy (range, 3-96) and abdominopelvic CT (range, 1-96). Tumor recurrence occurred in 167 patients (19.7%), of whom seven (4.2%) were locoregional recurrences in the peri-anastomotic area (n = 5) or regional gastric lymph nodes (n = 2). Whereas the peri-anastomotic recurrences were detected by both endoscopy and abdominopelvic CT, regional lymph node recurrences were only detected by abdominopelvic CT. Out of the 23 events of postoperative adverse events, the majority (87%) were detected by radiologic examinations; three events of benign strictures in the anastomotic site were detected only by endoscopy.
Endoscopic surveillance did not have a significant role in detecting locoregional tumor recurrence and postoperative adverse events after TG with R0 resection for gastric cancer. Routine endoscopic surveillance after TG may be considered optional and performed according to the capacities of each clinical setting.
胃癌全胃切除术后(TG)进行内镜监测以检测肿瘤复发和术后不良事件。然而,关于内镜监测临床益处的报道并不明确。我们研究了胃癌TG术后内镜监测的临床益处。
我们分析了2011年至2012年间接受胃癌R0切除TG的848例患者(380例早期胃癌和468例进展期胃癌),并接受了内镜和腹部盆腔增强计算机断层扫描(CT)的定期术后监测。
内镜检查(范围3 - 96个月)和腹部盆腔CT(范围1 - 96个月)的中位随访期均为58个月。167例患者(19.7%)发生肿瘤复发,其中7例(4.2%)为吻合口周围区域(n = 5)或区域胃淋巴结(n = 2)的局部复发。吻合口周围复发可通过内镜检查和腹部盆腔CT检测到,而区域淋巴结复发仅通过腹部盆腔CT检测到。在23例术后不良事件中,大多数(87%)通过影像学检查发现;3例吻合口良性狭窄仅通过内镜检查发现。
内镜监测在检测胃癌R0切除TG术后的局部肿瘤复发和术后不良事件方面没有显著作用。TG术后的常规内镜监测可视为可选择的,应根据各临床机构的能力进行。