Department of Thoracic Surgery, Choray Hospital, 202B Nguyen Chi Thanh Street, District No. 5, Hochiminh City, Vietnam.
J Cardiothorac Surg. 2021 Apr 13;16(1):77. doi: 10.1186/s13019-021-01455-5.
Recent developments in robotic technology have brought significant changes in robotic video-assisted thoracoscopic surgery (r-VATS) worldwide, particularly including the treatment in the thorax for the mediastinal, esophagus, and pulmonary lesions. Currently, there are only a few reports describing the procedural experience and outcomes with r-VATS. The objective of this study is to provide our initial experience using r-VATS at a single center, with specific attention to safety, efficacy, and procedural details.
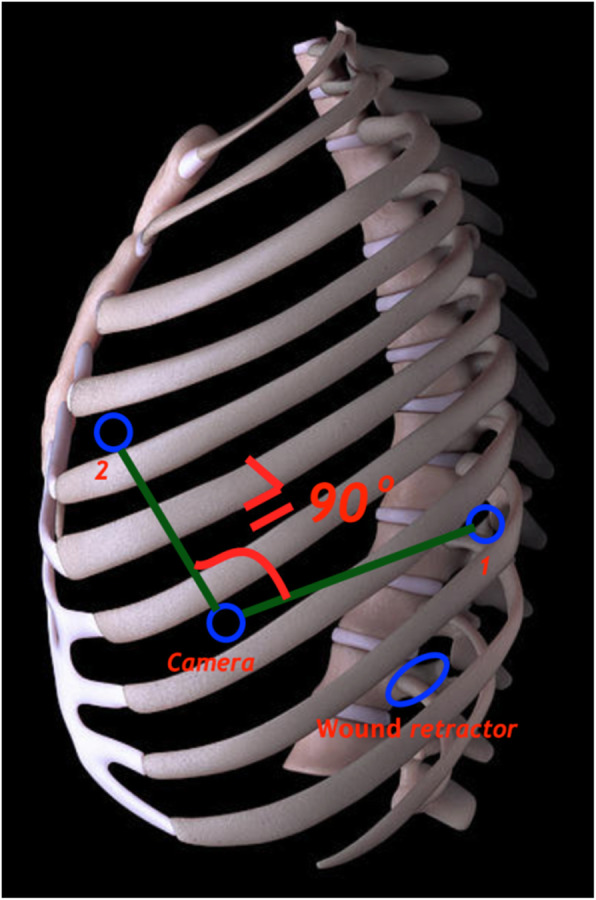
We retrospectively reviewed patients who underwent a newly modified r-VATS procedure for various surgical operations at the thoracic department of our hospital, from July 2018 to January 2020. Multiport trocars were placed in the classic triangular arrangement as in conventional VATS (c-VATS) but with modifications based on the type of surgery. The peri- and postoperative outcomes such as duration of surgery, complications, and duration of hospital stay for these patients were reported.
Overall, 142 patients underwent r-VATS for lobectomy (66), wedge resection (15), thymectomy (22), mediastinal tumor resection (30), pneumonectomy (4), transthoracic esophagectomy (1), esophageal tumor resection or esophageal diverticulum repair (2), diaphragm plication (1), and mediastinal tumor resection plus thymectomy (1). For the entire cohort, the median operative time was 110 min, and the median length of hospital stay was 5 days. Conversion to open thoracic surgery was reported only in a total of 3 (2.1%) patients of pneumonectomy (1.4%) and mediastinal tumor resection (0.70%). All our patients were managed successfully with no postoperative complications and mortality.
Our method of r-VATS was found to be safe and effective and may be applied to different surgical operations. Adequate and proper training of thoracic surgeons is immediately needed for the transition from c-VATS to r-VATS. The utility and advantages of triangular trocar configuration for r-VATS require further refinement and research before it can be routinely adopted in clinical practice.
Retrospectively registered.
近年来,机器人技术的发展在全球范围内带来了机器人辅助胸腔镜手术(r-VATS)的重大变革,特别是在治疗纵隔、食管和肺部病变方面。目前,只有少数报道描述了 r-VATS 的手术经验和结果。本研究的目的是提供我们在单一中心使用 r-VATS 的初步经验,特别关注安全性、有效性和手术细节。
我们回顾性分析了 2018 年 7 月至 2020 年 1 月我院胸外科接受新改良 r-VATS 手术的患者,这些手术包括各种外科手术。多端口套管针按传统胸腔镜手术(c-VATS)的经典三角形排列放置,但根据手术类型进行了修改。报告了这些患者的围手术期结果,如手术时间、并发症和住院时间。
总体而言,142 例患者接受 r-VATS 行肺叶切除术(66 例)、楔形切除术(15 例)、胸腺切除术(22 例)、纵隔肿瘤切除术(30 例)、肺切除术(4 例)、经胸食管切除术(1 例)、食管肿瘤切除术或食管憩室修复术(2 例)、膈折叠术(1 例)和纵隔肿瘤切除术加胸腺切除术(1 例)。对于整个队列,中位手术时间为 110 分钟,中位住院时间为 5 天。仅在 3 例(2.1%)肺切除术(1.4%)和纵隔肿瘤切除术(0.70%)中转开胸手术。我们所有的患者都成功地接受了治疗,没有术后并发症和死亡。
我们的 r-VATS 方法被证明是安全有效的,可应用于不同的手术。从 c-VATS 过渡到 r-VATS,需要对胸外科医生进行充分和适当的培训。在常规临床实践中采用三角套管针配置的 r-VATS 的实用性和优势需要进一步完善和研究。
回顾性注册。