Li Tian-En, Zhang Ze, Wang Yi, Xu Da, Dong Jian, Zhu Ying, Wang Zheng
Department of General Surgery, Qilu Hospital, Shandong University, Jinan 250012, China.
Department of General Surgery, Huashan Hospital & Cancer Metastasis Institute, Fudan University, Shanghai 200040, China.
J Cancer. 2021 Mar 15;12(10):2866-2876. doi: 10.7150/jca.54408. eCollection 2021.
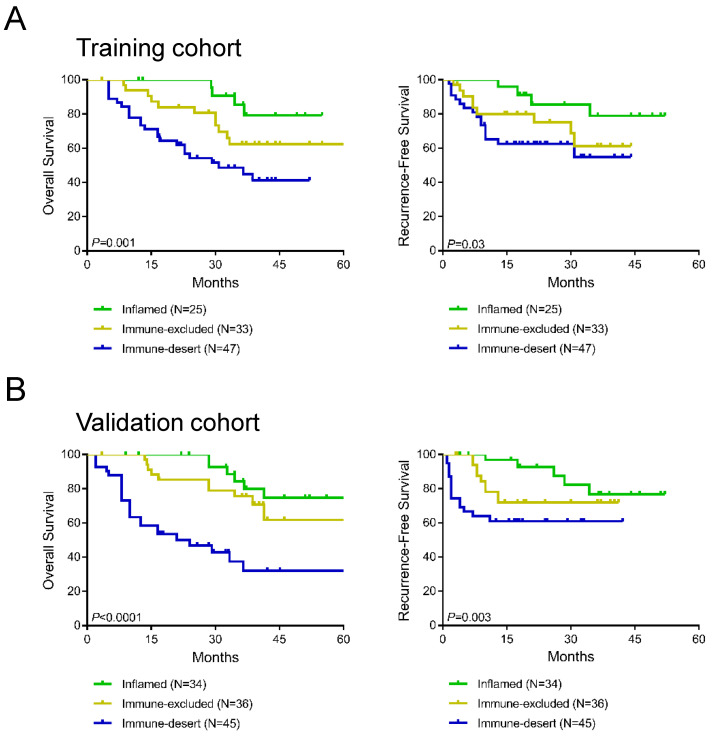
: The tumor microenvironment can be divided into inflamed, immune-excluded and immunedesert phenotypes according to CD8 T cell categories with differential programmed cell death protein 1 (PD-L1) expression. The study aims to construct a novel immunotype-based risk stratification model to predict postsurgical survival and adjuvant trans-arterial chemoembolization (TACE) response in patients with hepatocellular carcinoma (HCC). A total of 220 eligible HCC patients participated in this study. CD8 T cell infiltration and PD-L1 expression mode were estimated by immunohistochemical staining. A risk stratification model was developed and virtualized by a nomogram that integrated these independent prognostic factors. The postoperative prognosis and adjuvant TACE benefits were evaluated with a novel immunotype-based risk stratification model. A total of 220 patients were finally identified. Immune-desert, immune-excluded, and inflamed immunotypes represented 45%, 24%, and 31% of HCC, respectively. Univariate and multivariate analyses identified immunotype and PD-L1 expression mode as independent prognostic factors for overall survival time (OS) and recurrence-free survival time (RFS). The nomogram was constructed by integrating immunotype, PD-L1 expression, Barcelona Clinic Liver Cancer (BCLC) stage and tumor grade. The C-index was 0.794 in the training cohort and 0.813 in the validation cohort. A risk stratification system was constructed based on the nomogram classifying HCC patients into 3 risk groups. The average OS times in the low-risk, intermediate-risk and high-risk groups in all cohorts were 77.1 months (95% CI 71.4-82.9), 53.7 months (95% CI 48.2-59.2), and 25.6 months (95% CI 21.4-29.7), respectively. Further analysis showed that OS was significantly improved by adjuvant TACE in the low- and intermediate-risk groups (0.041 and =0.010, respectively) but not in the high-risk group (=0.398). A novel immunotype-based risk stratification model was built to predict postoperative prognosis and adjuvant TACE benefit in HCC patients. These tools can assist in building a more customized method of HCC treatment.
肿瘤微环境可根据程序性细胞死亡蛋白1(PD-L1)表达不同的CD8 T细胞类别分为炎症型、免疫排除型和免疫沙漠型表型。本研究旨在构建一种基于新型免疫分型的风险分层模型,以预测肝细胞癌(HCC)患者术后生存率及辅助性经动脉化疗栓塞术(TACE)疗效。共有220例符合条件的HCC患者参与本研究。通过免疫组化染色评估CD8 T细胞浸润及PD-L1表达模式。通过整合这些独立预后因素的列线图建立并虚拟了风险分层模型。采用基于新型免疫分型的风险分层模型评估术后预后及辅助性TACE疗效。最终共纳入220例患者。免疫沙漠型、免疫排除型和炎症型免疫表型分别占HCC的45%、24%和31%。单因素和多因素分析确定免疫分型和PD-L1表达模式为总生存时间(OS)和无复发生存时间(RFS)的独立预后因素。通过整合免疫分型、PD-L1表达、巴塞罗那临床肝癌(BCLC)分期和肿瘤分级构建列线图。训练队列的C指数为0.794,验证队列的C指数为0.813。基于列线图构建了一个风险分层系统,将HCC患者分为3个风险组。所有队列中低风险、中风险和高风险组的平均OS时间分别为77.1个月(95%CI 71.4 - 82.9)、53.7个月(95%CI 48.2 - 59.2)和25.6个月(95%CI 21.4 - 29.7)。进一步分析表明,辅助性TACE可使低风险和中风险组的OS显著改善(分别为0.041和 =0.010),但高风险组未改善(=0.398)。构建了一种基于新型免疫分型的风险分层模型,以预测HCC患者术后预后及辅助性TACE疗效。这些工具有助于建立更个性化的HCC治疗方法。