From the Global Medical Affairs, AbbVie Inc, North Chicago, Illinois.
Anesth Analg. 2021 Oct 1;133(4):826-835. doi: 10.1213/ANE.0000000000005504.
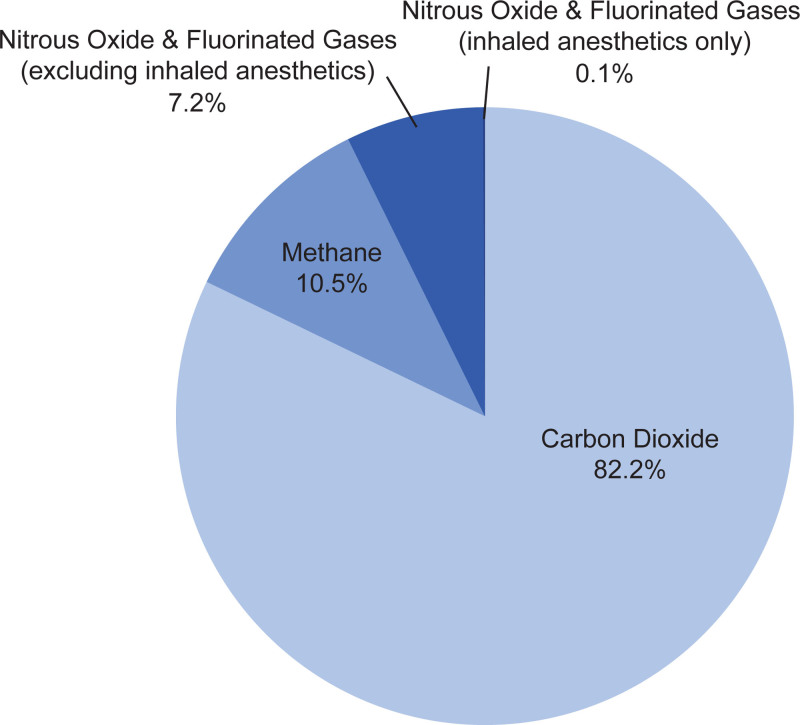
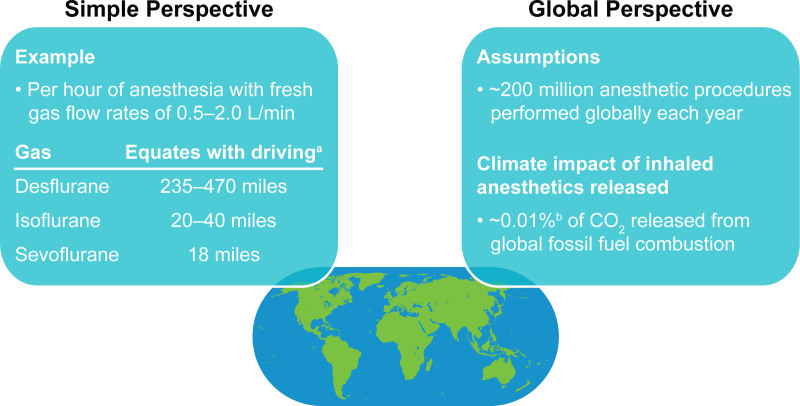
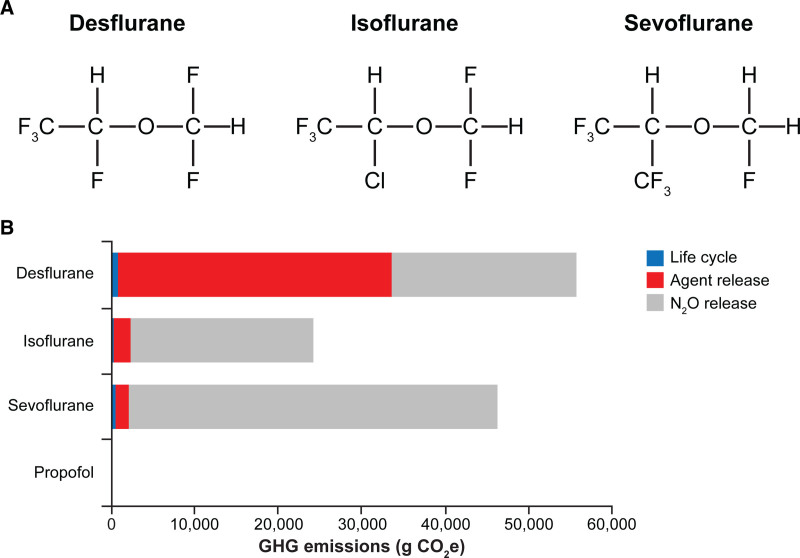
With an estimated worldwide volume of 266 million surgeries in 2015, the call for general inhalation anesthesia is considerable. However, widely used volatile anesthetics such as N2O and the highly fluorinated gases sevoflurane, desflurane, and isoflurane are greenhouse gases, ozone-depleting agents, or both. Because these agents undergo minimal metabolism in the body during clinical use and are primarily (≥95%) eliminated unchanged via exhalation, waste anesthetic gases (WAGs) in operating rooms and postanesthesia care units can pose a challenge for overall elimination and occupational exposure. The chemical properties and global warming impacts of these gases vary, with atmospheric lifetimes of 1-5 years for sevoflurane, 3-6 years for isoflurane, 9-21 years for desflurane, and 114 years for N2O. Additionally, the use of N2O as a carrier gas for the inhalation anesthetics and as a supplement to intravenous (IV) anesthetics further contributes to these impacts. At the same time, unscavenged WAGs can result in chronic occupational exposure of health care workers to potential associated adverse health effects. Few adverse effects associated with WAGs have been documented, however, when workplace exposure limits are implemented. Specific measures that can help reduce occupational exposure and the environmental impact of inhaled anesthetics include efficient ventilation and scavenging systems, regular monitoring of airborne concentrations of waste gases to remain below recommended limits, ensuring that anesthesia equipment is well maintained, avoiding desflurane and N2O if possible, and minimizing fresh gas flow rates (eg, use of low-flow anesthesia). One alternative to volatile anesthetics may be total intravenous anesthesia (TIVA). While TIVA is not associated with the risks of occupational exposure or atmospheric pollution that are inherent to volatile anesthetic gases, clinical considerations should be weighed in the choice of agent. Appropriate procedures for the disposal of IV anesthetics must be followed to minimize any potential for negative environmental effects. Overall, although their contributions are relatively low compared with those of other human-produced substances, inhaled anesthetics are intrinsically potent greenhouse gases and pose a risk to operating-room personnel if not properly managed and scavenged. Factors to reduce waste and minimize the future impact of these substances should be considered.
据估计,2015 年全球手术量为 2.66 亿例,因此对全身吸入麻醉的需求很大。然而,广泛使用的挥发性麻醉剂,如 N2O 以及高度氟化气体七氟醚、地氟醚和异氟醚,都是温室气体、消耗臭氧物质,或兼具两者。由于这些药物在临床应用中体内代谢很少,主要(≥95%)通过呼气以原形排出,手术室和麻醉后恢复室中的废气(WAGs)对整体消除和职业暴露构成挑战。这些气体的化学性质和全球变暖影响各不相同,其中七氟醚的大气寿命为 1-5 年,异氟醚为 3-6 年,地氟醚为 9-21 年,N2O 为 114 年。此外,N2O 被用作吸入麻醉剂的载体气体和静脉(IV)麻醉剂的补充剂,这进一步加剧了这些影响。与此同时,未清除的 WAGs 会导致医护人员慢性职业暴露于潜在相关的不良健康影响。然而,当实施工作场所暴露限制时,与 WAGs 相关的不良影响很少有记录。可以采取特定措施来帮助减少吸入麻醉剂的职业暴露和环境影响,包括高效通风和清除系统、定期监测废气的空气浓度以保持在建议的限制以下、确保麻醉设备得到良好维护、尽可能避免使用地氟醚和 N2O 以及尽量减少新鲜气体流量(例如,使用低流量麻醉)。挥发性麻醉剂的替代方法之一可能是全凭静脉麻醉(TIVA)。虽然 TIVA 与挥发性麻醉剂气体固有的职业暴露或大气污染风险无关,但在选择药物时应权衡临床考虑因素。必须遵循 IV 麻醉剂的适当处理程序,以将任何潜在的环境影响降到最低。总的来说,尽管与其他人为产生的物质相比,吸入麻醉剂的贡献相对较低,但它们是内在的强效温室气体,如果不妥善管理和清除,会对手术室人员构成风险。应考虑减少这些物质的浪费和最小化其未来影响的因素。