Department of Hematology, Oncology, and Tumor Immunology, Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Augustenburger Platz 1, Berlin 13353, Germany.
Department of Pathology and Tumor Biology, Graduate School of Medicine, Kyoto University, Kyoto, Japan.
EBioMedicine. 2021 Apr;66:103327. doi: 10.1016/j.ebiom.2021.103327. Epub 2021 Apr 13.
high recurrence rates of up to 75% within 2 years in pancreatic ductal adenocarcinoma (PDAC) patients resected for cure indicate a high medical need for clinical prediction tools and patient specific treatment approaches. Addition of the EGFR inhibitor erlotinib to adjuvant chemotherapy failed to improve outcome but its efficacy in some patients warrants predictors of responsiveness.
we analysed tumour samples from 293 R0-resected patients from the randomized, multicentre phase III CONKO-005 trial (gemcitabine ± erlotinib) with targeted sequencing, copy number, and RNA expression analyses.
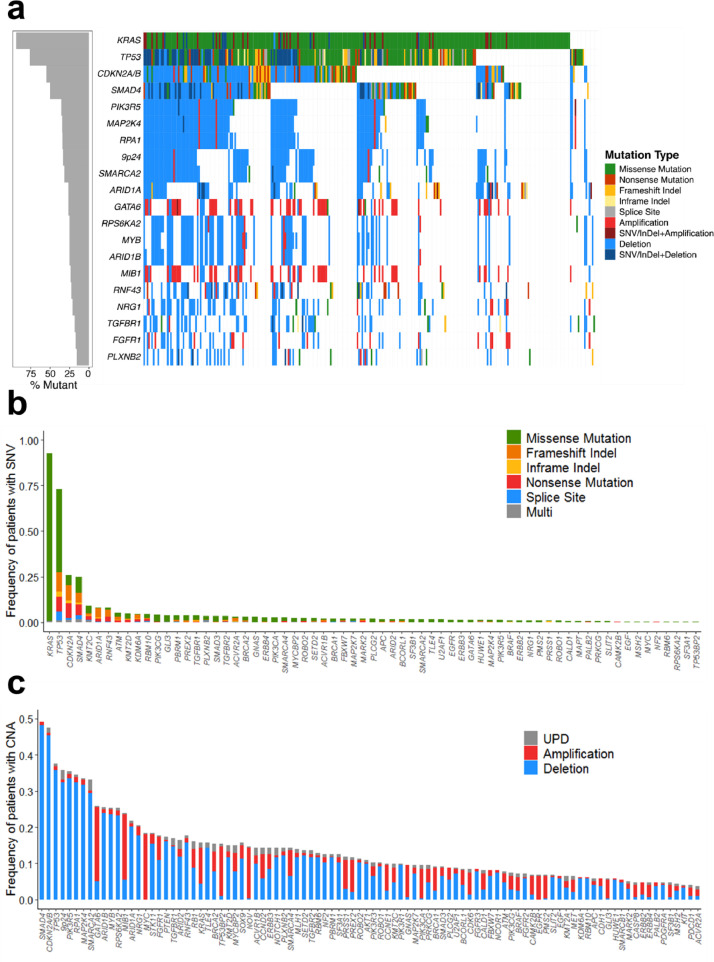
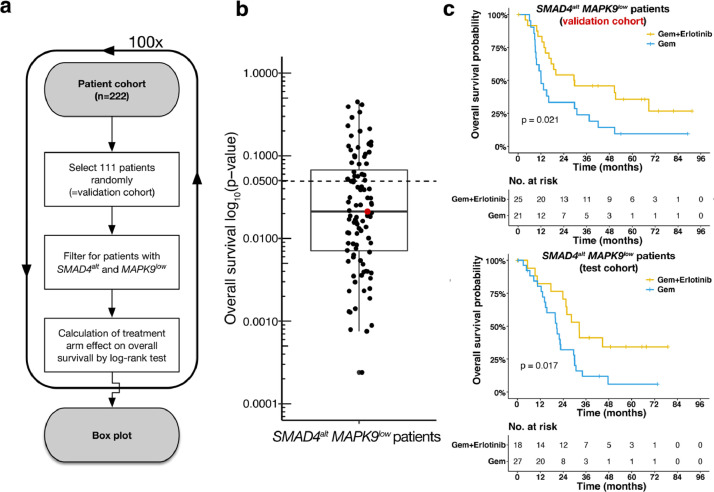
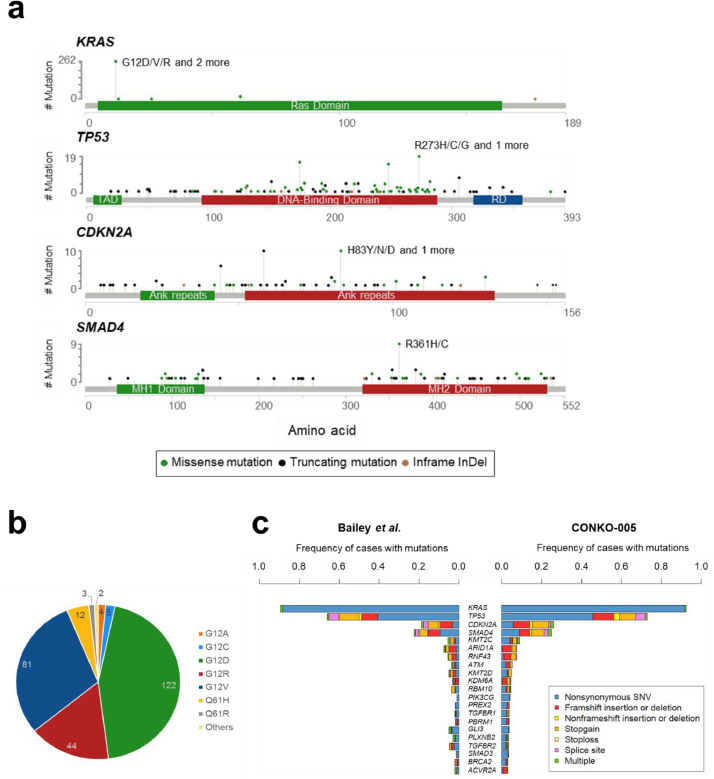
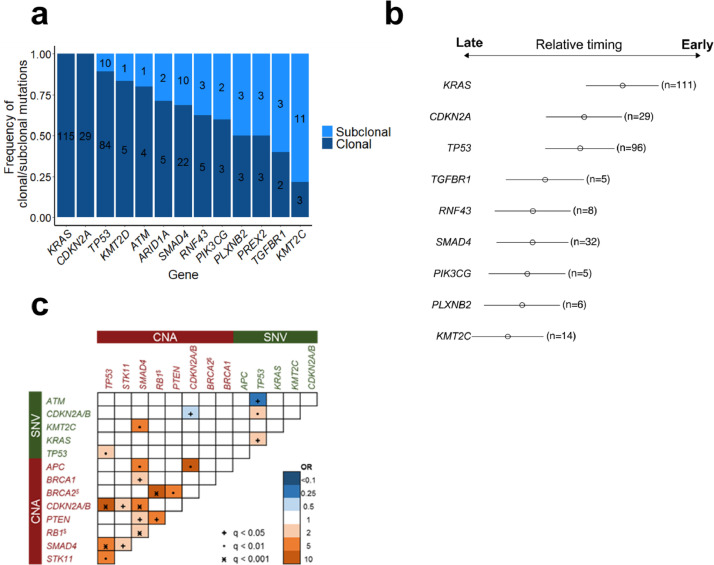
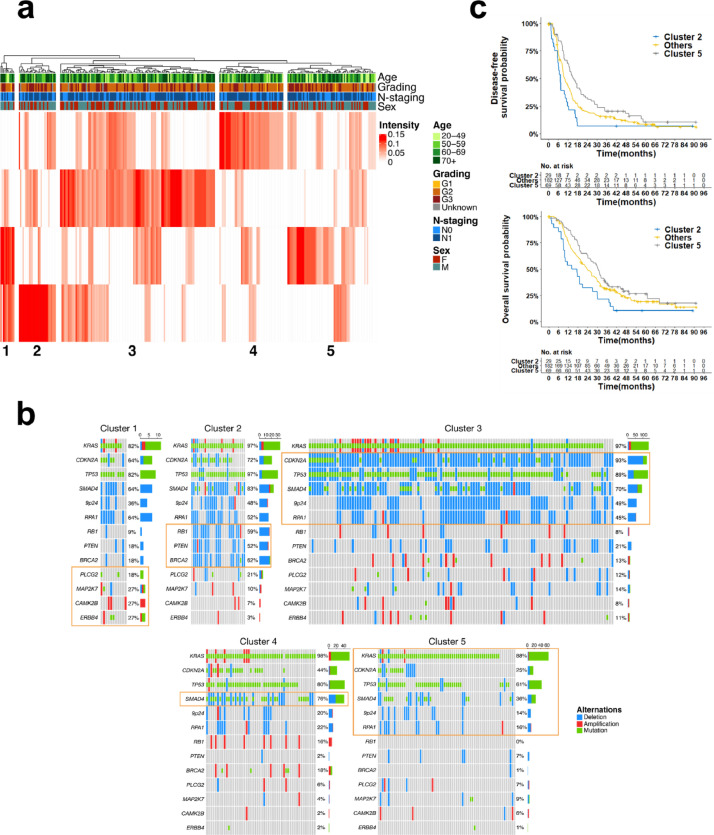
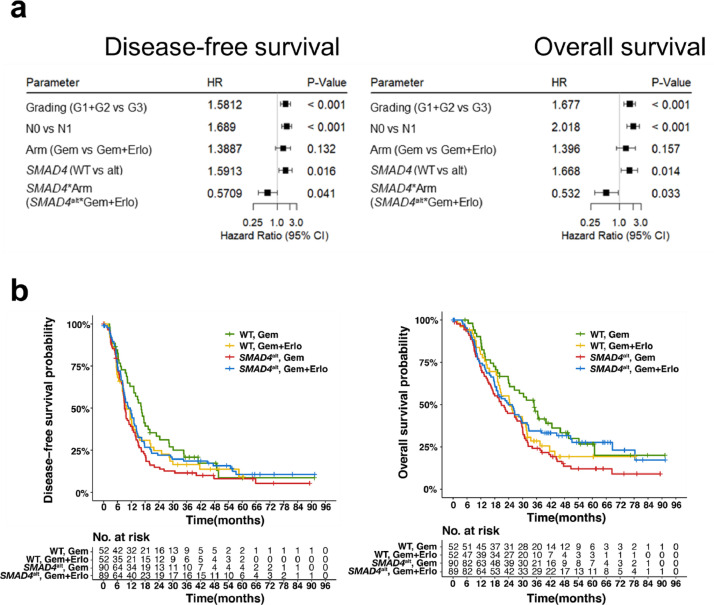
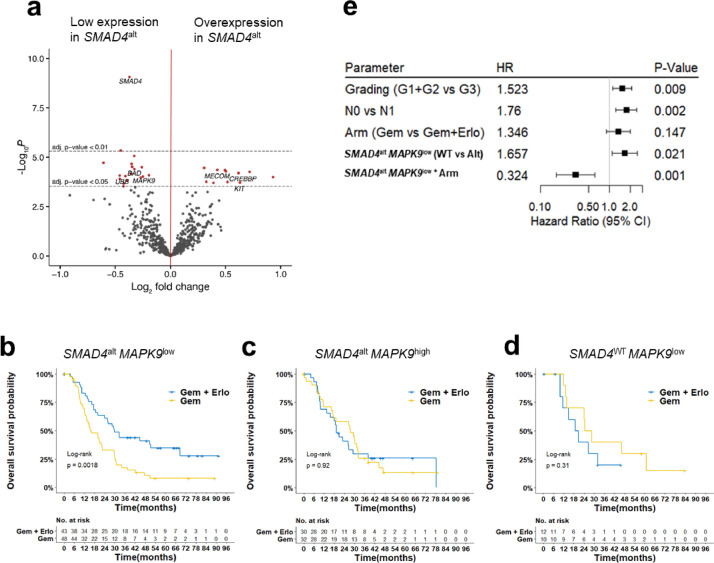
a total of 1086 mutations and 4157 copy-number aberrations (CNAs) with a mean of 17.9 /tumour were identified. Main pathways affected by genetic aberrations were the MAPK-pathway (99%), cell cycle control (92%), TGFβ signalling (77%), chromatin remodelling (71%), and the PI3K/AKT pathway (65%). Based on genetic signatures extracted with non-negative matrix factorization we could define five patient clusters, which differed in mutation patterns, gene expression profiles, and survival. In multivariable Cox regression analysis, SMAD4 aberrations were identified as a negative prognostic marker in the gemcitabine arm, an effect that was counteracted when treated with erlotinib (DFS: HR=1.59, p = 0.016, and OS: HR = 1.67, p = 0.014). Integration of differential gene expression analysis established SMAD4 alterations with low MAPK9 expression (n = 91) as a predictive biomarker for longer DFS (HR=0.49; test for interaction, p = 0.02) and OS (HR = 0.32; test for interaction, p = 0.001).
this study identified five biologically distinct patient clusters with different actionable lesions and unravelled a previously unappreciated association of SMAD4 alteration status with erlotinib effectiveness. Confirmatory studies and mechanistic experiments are warranted to challenge the hypothesis that SMAD4 status might guide addition of erlotinib treatment in early-stage PDAC patients.
在接受根治性手术的胰腺导管腺癌 (PDAC) 患者中,高达 75%的高复发率表明在 2 年内需要临床预测工具和针对患者的治疗方法。将表皮生长因子受体抑制剂厄洛替尼添加到辅助化疗中并未改善结局,但在一些患者中的疗效表明存在反应性的预测因子。
我们分析了来自随机、多中心 III 期 CONKO-005 试验(吉西他滨±厄洛替尼)中 293 例 R0 切除患者的肿瘤样本,进行了靶向测序、拷贝数和 RNA 表达分析。
共鉴定出 1086 个突变和 4157 个拷贝数异常(CNAs),每个肿瘤的平均数量为 17.9。受遗传异常影响的主要途径是 MAPK 途径(99%)、细胞周期控制(92%)、TGFβ 信号通路(77%)、染色质重塑(71%)和 PI3K/AKT 通路(65%)。基于非负矩阵分解提取的遗传特征,我们可以定义五个患者聚类,它们在突变模式、基因表达谱和生存方面存在差异。在多变量 Cox 回归分析中,SMAD4 异常被确定为吉西他滨组的负预后标志物,当用厄洛替尼治疗时,这种效应被抵消(DFS:HR=1.59,p=0.016,OS:HR=1.67,p=0.014)。差异基因表达分析的整合确定了 SMAD4 改变与低 MAPK9 表达(n=91)作为较长 DFS(HR=0.49;交互检验,p=0.02)和 OS(HR=0.32;交互检验,p=0.001)的预测生物标志物。
本研究鉴定了五个具有不同可操作病变的生物学上不同的患者聚类,并揭示了 SMAD4 改变状态与厄洛替尼疗效之间以前未被认识到的关联。需要进行验证性研究和机制实验来挑战 SMAD4 状态可能指导早期 PDAC 患者添加厄洛替尼治疗的假设。