Mitsui Suguru, Tauchi Shunsuke, Uchida Takahiro, Ohnishi Hisashi, Shimokawa Toshio, Tobe Satoshi
Department of Thoracic Surgery, Akashi Medical Center, 743-33 Okubocho Yagi, Akashi, Hyogo, 674-0063, Japan.
Department of Respiratory Medicine, Akashi Medical Center, Akashi, Japan.
J Cardiothorac Surg. 2021 Apr 21;16(1):105. doi: 10.1186/s13019-021-01485-z.
We investigated the most effective suction pressure for preventing or promptly improving postoperative air leaks on digital drainage devices after lung resection.
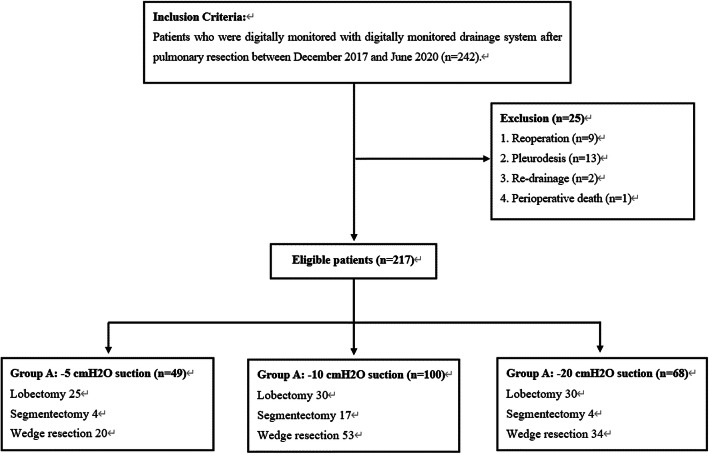
We retrospectively analyzed the postoperative data of 242 patients who were monitored with a digital drainage system after pulmonary resection in our institution between December 2017 and June 2020. We divided the patients into three groups according to the suction pressure used: A (low-pressure suction group: - 5 cm HO), B (intermediate-pressure group: - 10 cm HO), and C (high-pressure suction group: - 20 cm HO). We evaluated the duration of air leaks, timing of chest tube replacement, the amount of postoperative air leak, volume of fluid drained before chest tube removal, and the total number of air leaks during drainage.
In total, 217 patients were included in this study. The duration of air leaks gradually decreased with significant difference between the groups, the highest decrease in A, the lowest decrease in C (P = 0.019). Timing of chest tube replacement, on the other hand, did not significantly differ between the three groups (P = 0.126). The number of postoperative air leaks just after surgery did not significantly differ between the three groups (P = 0.175), but the number of air leaks on postoperative day 1 were fewest in group A, then B, and greatest in group C (P = 0.033). The maximum amount of air leaks during drainage was lowest in A, then B, and highest in C (P = 0.036). Volume of fluid drained before chest tube removal did not significantly differ between the three groups (P = 0.986).
Low-pressure suction after pulmonary resection seems to avoid or promptly improve postoperative air leaks in digital drainage devices after lung resection.
This is a single-institution, retrospective analysis-based study of data from an electronic database. Study protocol was approved by the Akashi Medical Center Institutional Research Ethics Board (approval number: 2020-9).
我们研究了在肺切除术后数字引流装置上预防或迅速改善术后漏气的最有效吸引压力。
我们回顾性分析了2017年12月至2020年6月期间在我院接受肺切除术后使用数字引流系统监测的242例患者的术后数据。我们根据使用的吸引压力将患者分为三组:A组(低压吸引组:-5cmH₂O)、B组(中压组:-10cmH₂O)和C组(高压吸引组:-20cmH₂O)。我们评估了漏气持续时间、胸管更换时间、术后漏气量、胸管拔除前引流的液体量以及引流期间漏气的总数。
本研究共纳入217例患者。漏气持续时间逐渐缩短,组间差异有统计学意义,A组下降幅度最大,C组下降幅度最小(P = 0.019)。另一方面,三组间胸管更换时间无显著差异(P = 0.126)。术后刚手术时的术后漏气次数在三组间无显著差异(P = 0.175),但术后第1天的漏气次数A组最少,其次是B组,C组最多(P = 0.033)。引流期间漏气的最大量A组最低,其次是B组,C组最高(P = 0.036)。胸管拔除前引流的液体量在三组间无显著差异(P = 0.986)。
肺切除术后低压吸引似乎可避免或迅速改善肺切除术后数字引流装置的术后漏气。
这是一项基于单机构电子数据库数据的回顾性分析研究。研究方案已获得明石医疗中心机构研究伦理委员会批准(批准号:2020 - 9)。