Lymphoid Malignancies Branch, Center for Cancer Research, National Cancer Institute, Bethesda, Maryland, USA.
Department of Laboratory Medicine, NIH Clinical Center, Bethesda, Maryland, USA.
J Immunother Cancer. 2021 Apr;9(4). doi: 10.1136/jitc-2020-002193.
Full application of cytokines as oncoimmunotherapeutics requires identification of optimal regimens. Our initial effort with intravenous bolus recombinant human interleukin-15 (rhIL-15) was limited by postinfusional reactions. Subcutaneous injection and continuous intravenous infusion for 10 days (CIV-10) provided rhIL-15 with less toxicity with CIV-10 giving the best increases in CD8 lymphocytes and natural killer (NK) cells. To ease rhIL-15 administration, we shortened time of infusion. Treatment with rhIL-15 at a dose of 3-5 µg/kg as a 5-day continuous intravenous infusion (CIV-5) had no dose-limiting toxicities while effector cell stimulation was comparable to the CIV-10 regimen.
Eleven patients with metastatic cancers were treated with rhIL-15 CIV-5, 3 µg (n=4), 4 µg (n=3), and 5 µg/kg/day (n=4) in a phase I dose-escalation study (April 6, 2012).
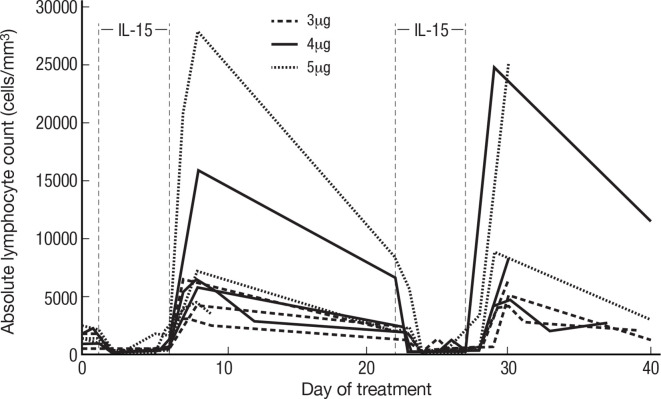
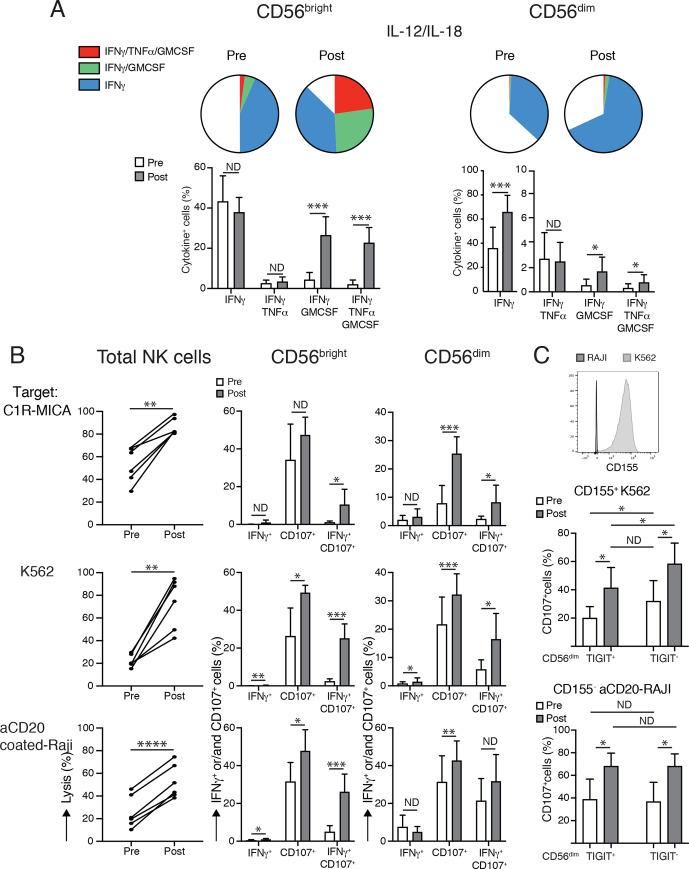
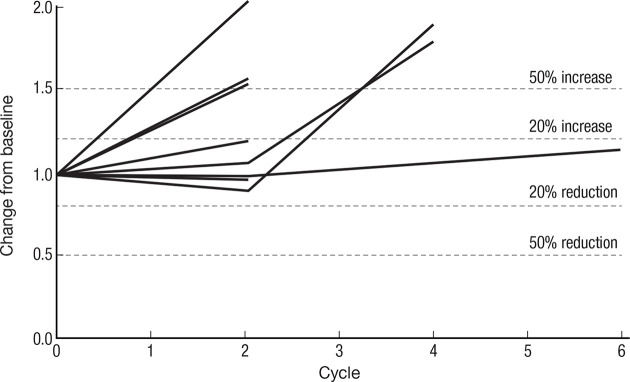
Impressive expansions of NK cells were seen at all dose levels (mean 34-fold), including CD56 NK cells (mean 144-fold for 4 µg/kg), as well as an increase in CD8 T cells (mean 3.38-fold). At 5 µg/kg/day, there were no dose-limiting toxicities but pulmonary capillary leak and slower patient recovery. This led to our choice of the 4 µg/kg as CIV-5 dose for further testing. Cytolytic capacity of CD56 and CD56 NK cells was increased by interleukin-15 assayed by antibody-dependent cellular cytotoxicity (ADCC), natural cytotoxicity and natural killer group 2D-mediated cytotoxicity. The best response was stable disease.
IL-15 administered as CIV-5 substantially expanded NK cells with increased cytotoxic functions. Tumor-targeting monoclonal antibodies dependent on ADCC as their mechanism of action including alemtuzumab, obinutuzumab, avelumab, and mogamulizumab could benefit from those NK cell expansions and provide a promising therapeutic strategy.
NCT01572493, NCT03759184, NCT03905135, NCT04185220 and NCT02689453.
充分应用细胞因子作为肿瘤免疫治疗需要确定最佳方案。我们最初使用静脉推注重组人白细胞介素-15(rhIL-15)的尝试受到输注后反应的限制。皮下注射和连续静脉输注 10 天(CIV-10)使 rhIL-15 的毒性降低,而 CIV-10 使 CD8 淋巴细胞和自然杀伤(NK)细胞的增加最佳。为了便于 rhIL-15 的给药,我们缩短了输注时间。rhIL-15 以 3-5 µg/kg 的剂量连续静脉输注 5 天(CIV-5),没有剂量限制毒性,而效应细胞刺激与 CIV-10 方案相当。
11 名转移性癌症患者参加了一项 I 期剂量递增研究(2012 年 4 月 6 日),分别接受 rhIL-15 CIV-5 治疗,剂量为 3µg(n=4)、4µg(n=3)和 5µg/kg/天(n=4)。
在所有剂量水平上均观察到 NK 细胞的显著扩增(平均 34 倍),包括 CD56 NK 细胞(4µg/kg 时平均 144 倍),以及 CD8 T 细胞的增加(平均 3.38 倍)。5µg/kg/天时,无剂量限制毒性,但有肺毛细血管渗漏和患者恢复较慢。这导致我们选择 4µg/kg 作为 CIV-5 的剂量进行进一步测试。通过抗体依赖性细胞毒性(ADCC)测定的白细胞介素-15 扩增的 CD56 和 CD56 NK 细胞的细胞溶解能力增加,自然细胞毒性和自然杀伤组 2D 介导的细胞毒性。最佳反应是疾病稳定。
静脉滴注 5 天的 IL-15 可显著扩增 NK 细胞,并增强其细胞毒性功能。依赖 ADCC 作为其作用机制的肿瘤靶向单克隆抗体,包括阿仑单抗、奥滨尤妥珠单抗、avelumab 和 mogamulizumab,可能受益于这些 NK 细胞扩增,并提供一种有前途的治疗策略。
NCT01572493、NCT03759184、NCT03905135、NCT04185220 和 NCT02689453。