Department of Pathology, The Johns Hopkins University, Baltimore, Maryland.
Department of Obstetrics and Gynecology and Women's Health, Montefiore Medical Center, Albert Einstein College of Medicine, Bronx, New York.
Clin Cancer Res. 2021 Sep 15;27(18):4953-4973. doi: 10.1158/1078-0432.CCR-20-2833. Epub 2021 Apr 22.
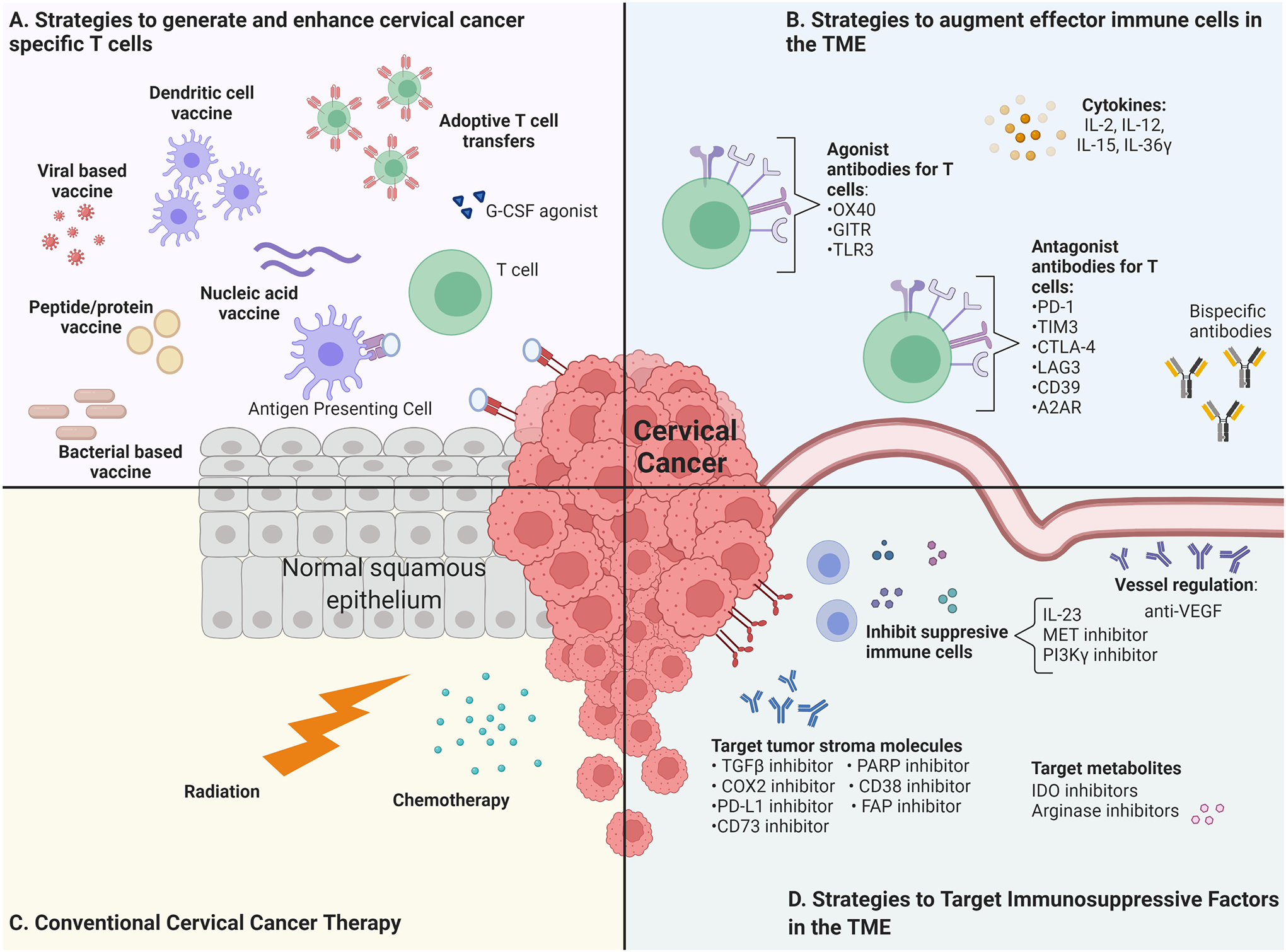
It is a sad fact that despite being almost completely preventable through human papillomavirus (HPV) vaccination and screening, cervical cancer remains the fourth most common cancer to affect women worldwide. Persistent high-risk HPV (hrHPV) infection is the primary etiologic factor for cervical cancer. Upward of 70% of cases are driven by HPV types 16 and 18, with a dozen other hrHPVs associated with the remainder of cases. Current standard-of-care treatments include radiotherapy, chemotherapy, and/or surgical resection. However, they have significant side effects and limited efficacy against advanced disease. There are a few treatment options for recurrent or metastatic cases. Immunotherapy offers new hope, as demonstrated by the recent approval of programmed cell death protein 1-blocking antibody for recurrent or metastatic disease. This might be augmented by combination with antigen-specific immunotherapy approaches, such as vaccines or adoptive cell transfer, to enhance the host cellular immune response targeting HPV-positive cancer cells. As cervical cancer progresses, it can foster an immunosuppressive microenvironment and counteract host anticancer immunity. Thus, approaches to reverse suppressive immune environments and bolster effector T-cell functioning are likely to enhance the success of such cervical cancer immunotherapy. The success of nonspecific immunostimulants like imiquimod against genital warts also suggest the possibility of utilizing these immunotherapeutic strategies in cervical cancer prevention to treat precursor lesions (cervical intraepithelial neoplasia) and persistent hrHPV infections against which the licensed prophylactic HPV vaccines have no efficacy. Here, we review the progress and challenges in the development of immunotherapeutic approaches for the prevention and treatment of cervical cancer.
尽管人乳头瘤病毒 (HPV) 疫苗接种和筛查几乎可以完全预防宫颈癌,但它仍是全球女性中第四种最常见的癌症。持续性高危型 HPV(hrHPV)感染是宫颈癌的主要病因。超过 70%的病例由 HPV 16 和 18 型驱动,其余由 12 种其他 hrHPV 型引起。目前的标准治疗方法包括放疗、化疗和/或手术切除。然而,它们对晚期疾病的疗效有限,且具有显著的副作用。对于复发性或转移性病例,有几种治疗选择。免疫疗法带来了新的希望,最近批准的程序性细胞死亡蛋白 1 阻断抗体用于复发性或转移性疾病就是例证。通过与抗原特异性免疫疗法(如疫苗或过继性细胞转移)联合使用,增强针对 HPV 阳性癌细胞的宿主细胞免疫反应,可能会增强这种宫颈癌免疫疗法的效果。随着宫颈癌的进展,它会形成免疫抑制微环境,从而对抗宿主的抗癌免疫。因此,逆转抑制性免疫环境和增强效应 T 细胞功能的方法可能会增强这种宫颈癌免疫疗法的成功。非特异性免疫刺激剂咪喹莫特对生殖器疣的成功也表明,有可能利用这些免疫治疗策略在宫颈癌预防中治疗前病变(宫颈上皮内瘤变)和持续性 hrHPV 感染,而已上市的预防性 HPV 疫苗对这些感染无效。在此,我们综述了免疫治疗方法在预防和治疗宫颈癌方面的进展和挑战。