Ieiri Satoshi, Nagata Kouji
Department of Pediatric Surgery, Research Field in Medical and Health Sciences, Medical and Dental Area, Research and Education Assembly, Kagoshima University, 8-35-1, Sakuragaoka, Kagoshima, 890-8520, Japan.
Department of Pediatric Surgery, Faculty of Medical Sciences, Kyushu University, Fukuoka, Japan.
Surg Case Rep. 2021 Apr 23;7(1):103. doi: 10.1186/s40792-021-01190-y.
Pediatric hydronephrosis induced by pelvic-ureteric junction obstruction (PUJO) is treated by dismembered pyeloplasty (DP) via open and laparoscopic surgery. The etiology of PUJO involves both intrinsic stenosis and extrinsic compression of crossing vessels (CVs). PUJO owing to CVs is also treated by DP, as there is no consensus concerning this vascular condition. We encountered a 2-year-old infant with pure extrinsic PUJO combined with horseshoe kidney who successfully underwent laparoscopic transposition for CVs (vascular hitch).
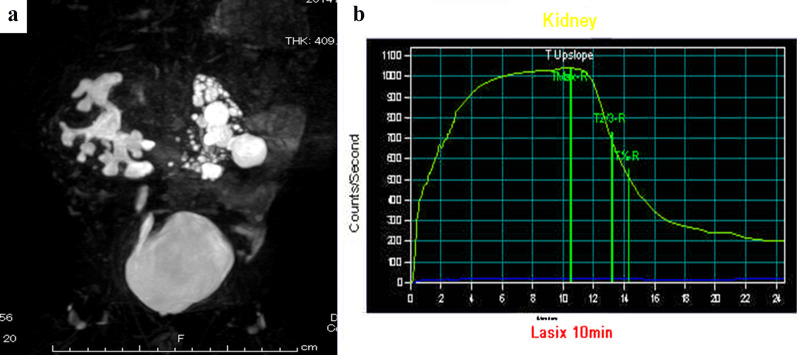
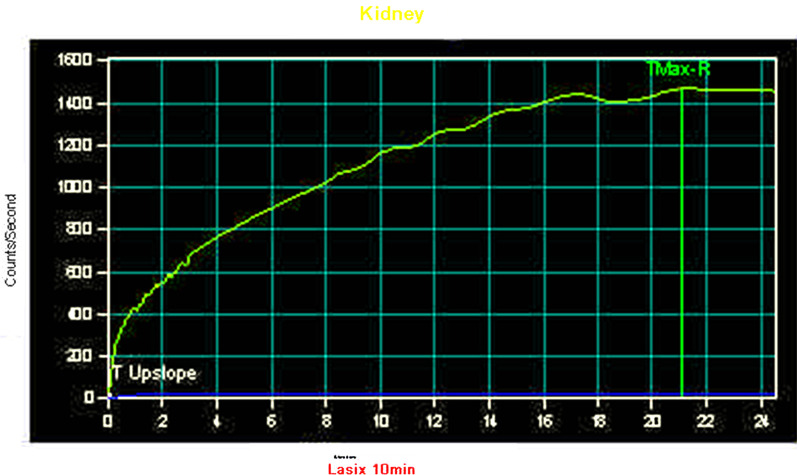
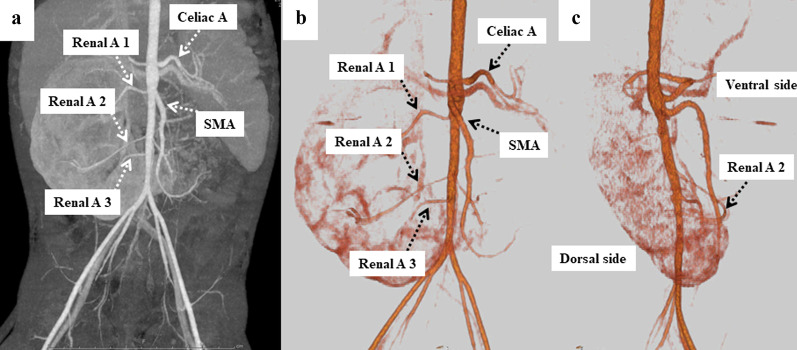
A 2-year-old boy was prenatally diagnosed with left multicystic dysplastic kidney (MDCK) and right hydronephrosis and received a definitive diagnosis after birth. At 6 months old, renal scintigraphy revealed a non-functioning pattern in the left kidney and an obstructive pattern in the right, showing no response to furosemide loading. The patient also had recurrent urinary tract infection, and his right hydronephrosis gradually worsened. We decided to perform surgery for the right PUJO. Preoperative enhanced computed tomography detected three right renal vessels independently branching from the abdominal aorta. The middle renal vessels were located at the ventral side of the pelvis and coincident with the site of PUJO. These vessels were suspected of being CVs. The patient underwent laparoscopic surgery electively. A 5-mm trocar was inserted at the umbilicus for a 5-mm, 30° rigid scope. Two additional ports were then inserted under laparoscope inspection. The dilated right pelvis and CVs were detected after ascending colon mobilization. To confirm the pathogenesis of PUJO, the CVs were dissected and taped. After taping the CVs, an intraoperative diuretic test was performed using furosemide loading. Peristalsis of the right ureter was recognized, and the extrinsic PUJO owing to the CVs was definitively confirmed. We therefore performed transposition for the CVs (vascular hitch procedure). The CVs were mobilized in the cranial direction and those were wrapped by dilated pelvis. The post-operative course was uneventful. The renal scintigraphy findings improved and showed a favorable response of furosemide loading.
The laparoscopic vascular hitch procedure is minimally invasive and effective for extrinsic PUJO due to CVs. Anastomotic stricture after Anderson and Hynes DP can be prevented by appropriate patient selection.
盆腔输尿管连接部梗阻(PUJO)所致小儿肾积水通过开放手术和腹腔镜手术行离断性肾盂成形术(DP)治疗。PUJO的病因包括内在狭窄和交叉血管(CVs)的外在压迫。由于CVs导致的PUJO也通过DP治疗,因为对于这种血管情况尚无共识。我们遇到一名2岁婴儿,患有单纯性外在性PUJO合并马蹄肾,成功接受了腹腔镜下CVs转位术(血管套叠术)。
一名2岁男孩产前诊断为左多囊性发育不良肾(MDCK)和右肾积水,出生后确诊。6个月大时,肾闪烁显像显示左肾无功能模式,右肾为梗阻模式,对呋塞米负荷试验无反应。该患者还反复发生尿路感染,右肾积水逐渐加重。我们决定对右PUJO进行手术。术前增强计算机断层扫描检测到三条右肾血管独立于腹主动脉分支。中间肾血管位于盆腔腹侧,与PUJO部位一致。怀疑这些血管为CVs。患者择期接受腹腔镜手术。在脐部插入一个5毫米套管针用于5毫米、30°硬镜。然后在腹腔镜检查下再插入另外两个端口。升结肠游离后检测到扩张的右肾盂和CVs。为确认PUJO的发病机制,对CVs进行解剖并结扎。结扎CVs后,使用呋塞米负荷进行术中利尿试验。观察到右输尿管蠕动,明确证实了由于CVs导致的外在性PUJO。因此,我们对CVs进行了转位术(血管套叠手术)。将CVs向头侧游离,并用扩张的肾盂包裹。术后过程顺利。肾闪烁显像结果改善,对呋塞米负荷试验显示良好反应。
腹腔镜血管套叠术对于由CVs导致的外在性PUJO微创且有效。通过适当选择患者可预防安德森和海因斯DP术后的吻合口狭窄。