Departments of Anaesthesiology, Intensive Care and Pain Medicine and Clinical Chemistry.
Department of Anaesthesiology, Intensive Care and Emergency Medicine, University Medical Centre Utrecht, Utrecht, The Netherlands.
BJS Open. 2021 Mar 5;5(2). doi: 10.1093/bjsopen/zrab015.
Cardiac and inflammatory biomarkers have been associated with adverse outcome after major abdominal surgery. This study investigated the effect of remote ischaemic preconditioning (RIPC) on perioperative concentrations of high-sensitive cardiac troponin (hs-cTn) T and interleukin (IL) 6.
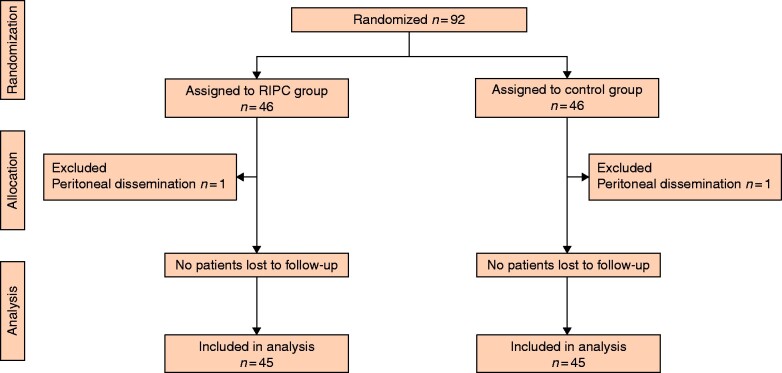
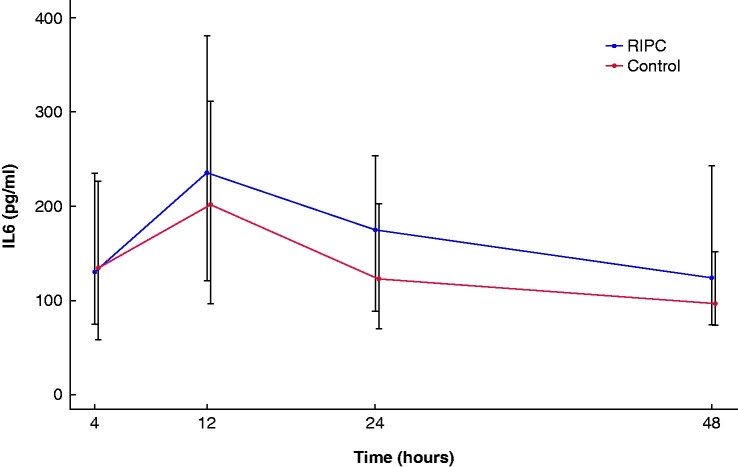
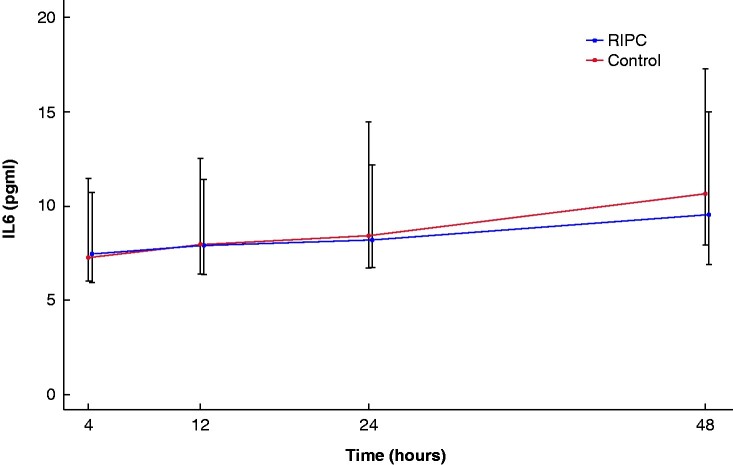
Adult patients scheduled for elective pancreatic surgery between March 2017 and February 2019 were randomized to either three cycles of upper-limb ischaemia and reperfusion (each 5 min) or a sham procedure before surgery. The primary endpoint was the maximum postoperative hs-cTnT concentration within 48 h after surgery. Secondary endpoints were postoperative myocardial injury (PMI), defined as an absolute increase of hs-cTnT of at least 14 ng/l above baseline concentration, maximum concentration of IL-6 within 48 h after surgery and postoperative complications within 30 days of surgery.
Of 99 eligible patients, 46 underwent RIPC and 46 a sham procedure. RIPC did not reduce the maximum hs-cTnT concentration after surgery (12.6 ng/l RIPC, 16.6 ng/l controls, P = 0.225), nor did it lessen the incidence of PMI (15/45 RIPC, 18/45 controls, P = 0.375). The maximum postoperative IL-6 concentration was 265 pg/ml after RIPC versus 385 pg/ml in controls (P = 0.108). Postoperative complications occurred in 23 RIPC and 24 control patients respectively.
Remote ischaemic preconditioning did not reduce the maximum postoperative hs-cTnT concentration. Postoperative myocardial injury, IL-6 concentrations and postoperative complications were similar between RIPC patients and controls.
Clinicaltrials.gov identifier NCT03460938.
心脏和炎症生物标志物与大腹部手术后的不良预后相关。本研究调查了远程缺血预处理(RIPC)对围手术期高敏心肌肌钙蛋白(hs-cTn)T 和白细胞介素(IL)6 浓度的影响。
2017 年 3 月至 2019 年 2 月期间,择期行胰腺手术的成年患者被随机分为三组,分别接受三组上肢缺血再灌注(每组 5 分钟)或手术前假处理。主要终点是手术后 48 小时内的最大术后 hs-cTnT 浓度。次要终点是术后心肌损伤(PMI),定义为 hs-cTnT 绝对增加至少 14ng/l 高于基线浓度,术后 48 小时内的最大 IL-6 浓度以及术后 30 天内的并发症。
99 例符合条件的患者中,46 例接受了 RIPC,46 例接受了假处理。RIPC 并未降低手术后的最大 hs-cTnT 浓度(12.6ng/l RIPC,16.6ng/l 对照组,P=0.225),也未降低 PMI 的发生率(15/45 RIPC,18/45 对照组,P=0.375)。RIPC 组术后最大 IL-6 浓度为 265pg/ml,对照组为 385pg/ml(P=0.108)。RIPC 组和对照组分别有 23 例和 24 例患者发生术后并发症。
远程缺血预处理不能降低术后 hs-cTnT 浓度的最大值。术后心肌损伤、IL-6 浓度和术后并发症在 RIPC 患者和对照组之间相似。
Clinicaltrials.gov 标识符 NCT03460938。