Autonomic Medicine Section, Clinical Neurosciences Program, Division of Intramural Research, National Institute of Neurological Disorders and Stroke, National Institutes of Health, Bethesda, MD, USA.
J Neurochem. 2021 Jul;158(2):554-568. doi: 10.1111/jnc.15371. Epub 2021 May 21.
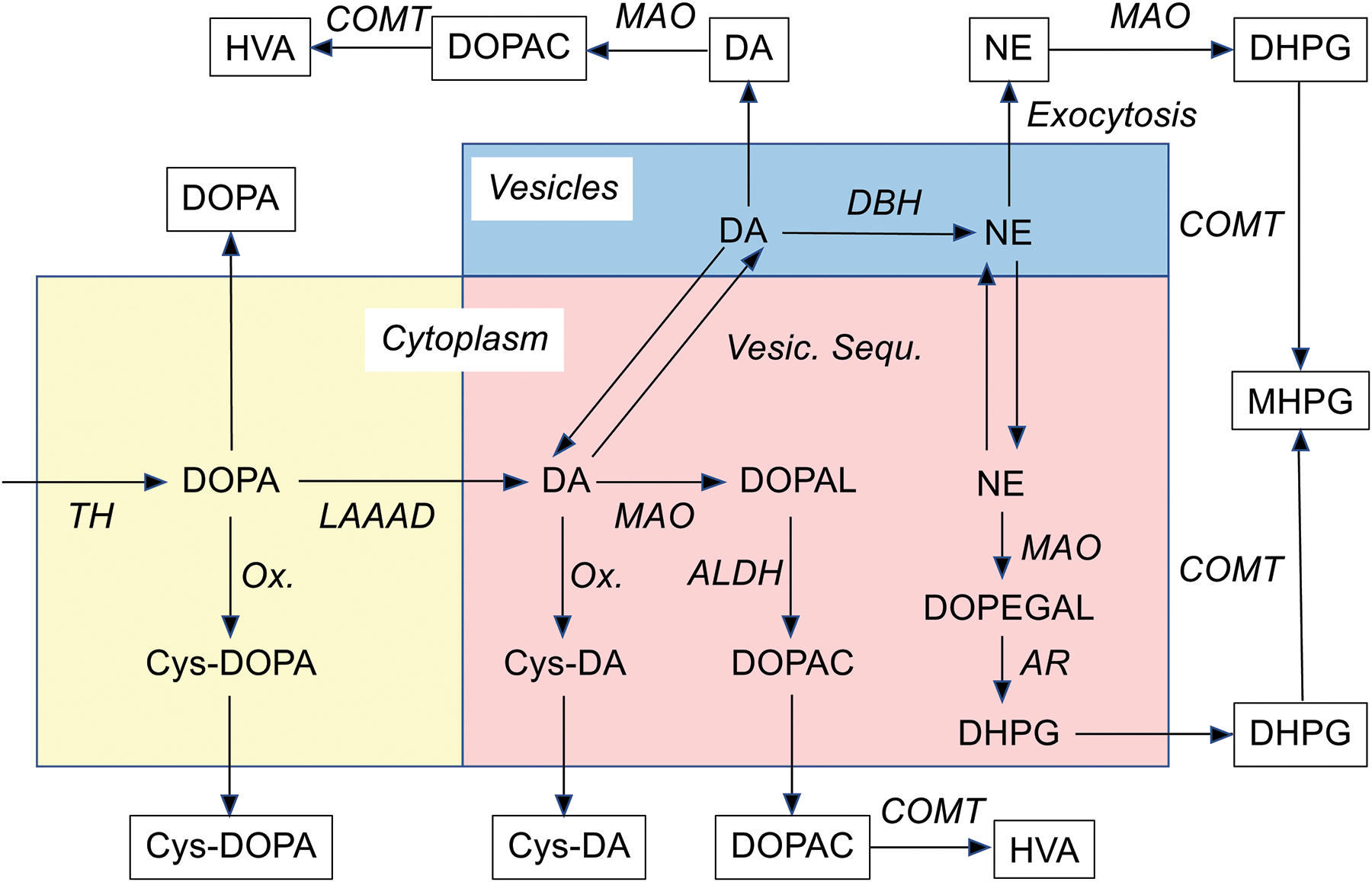
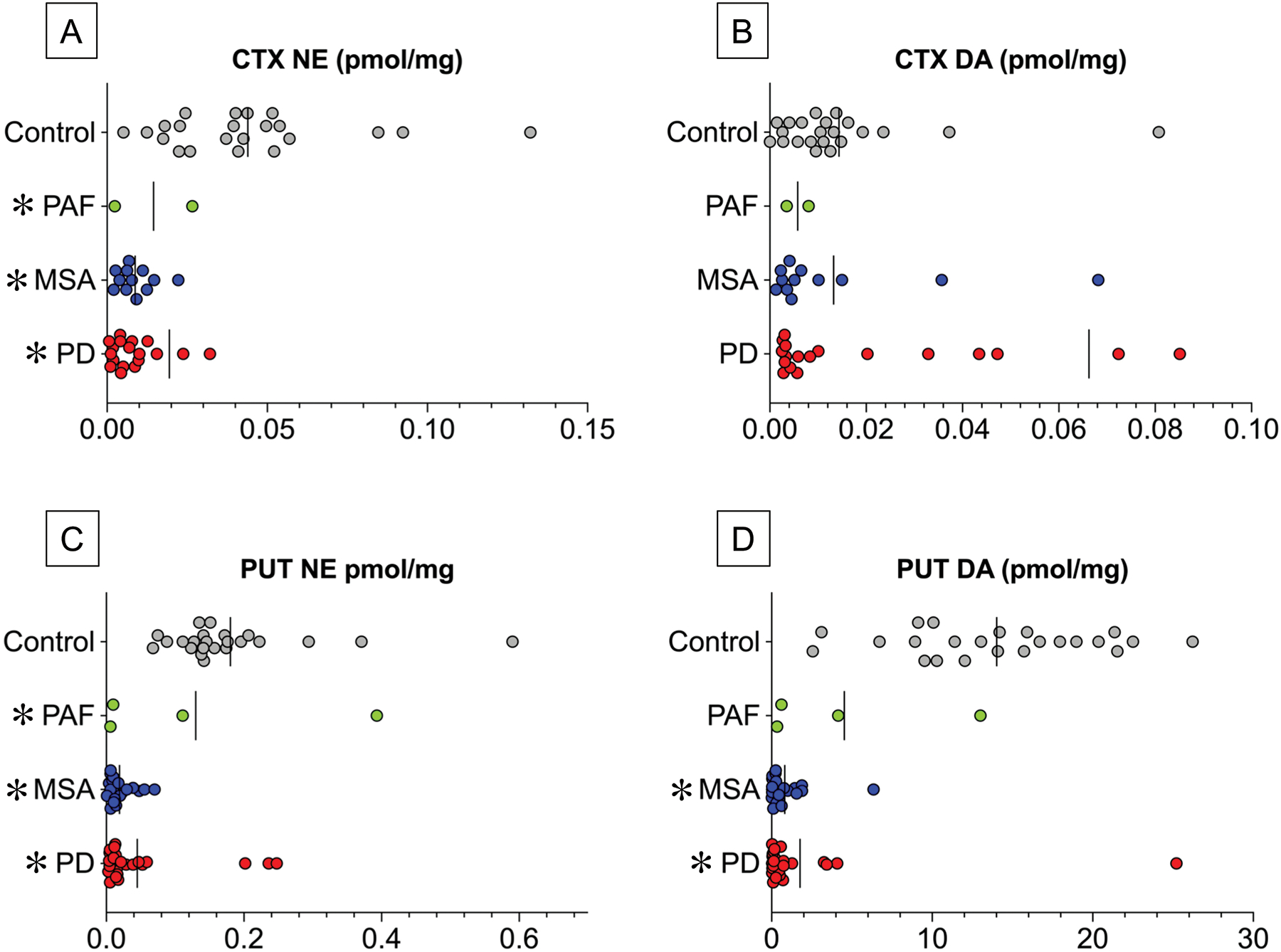
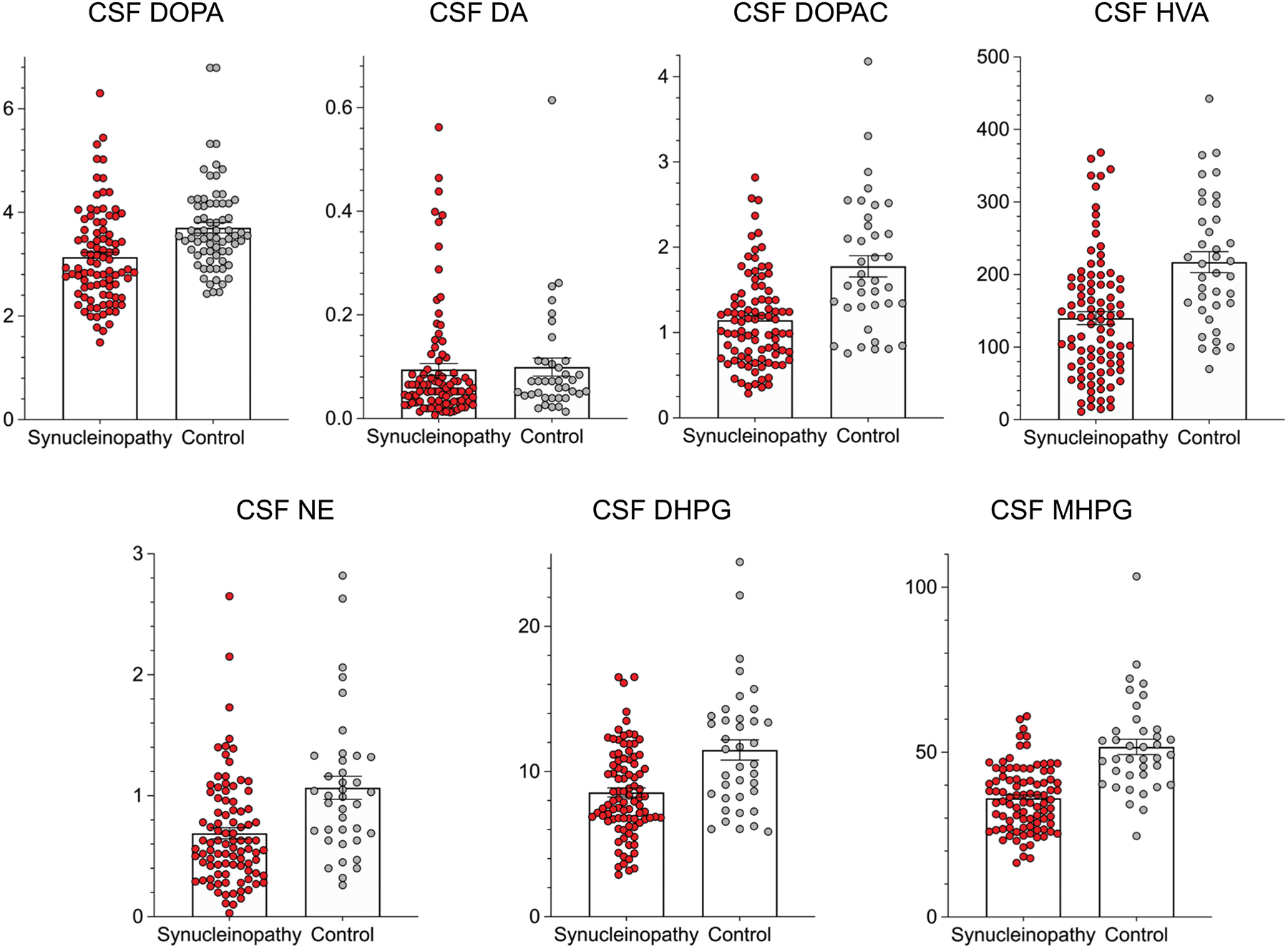
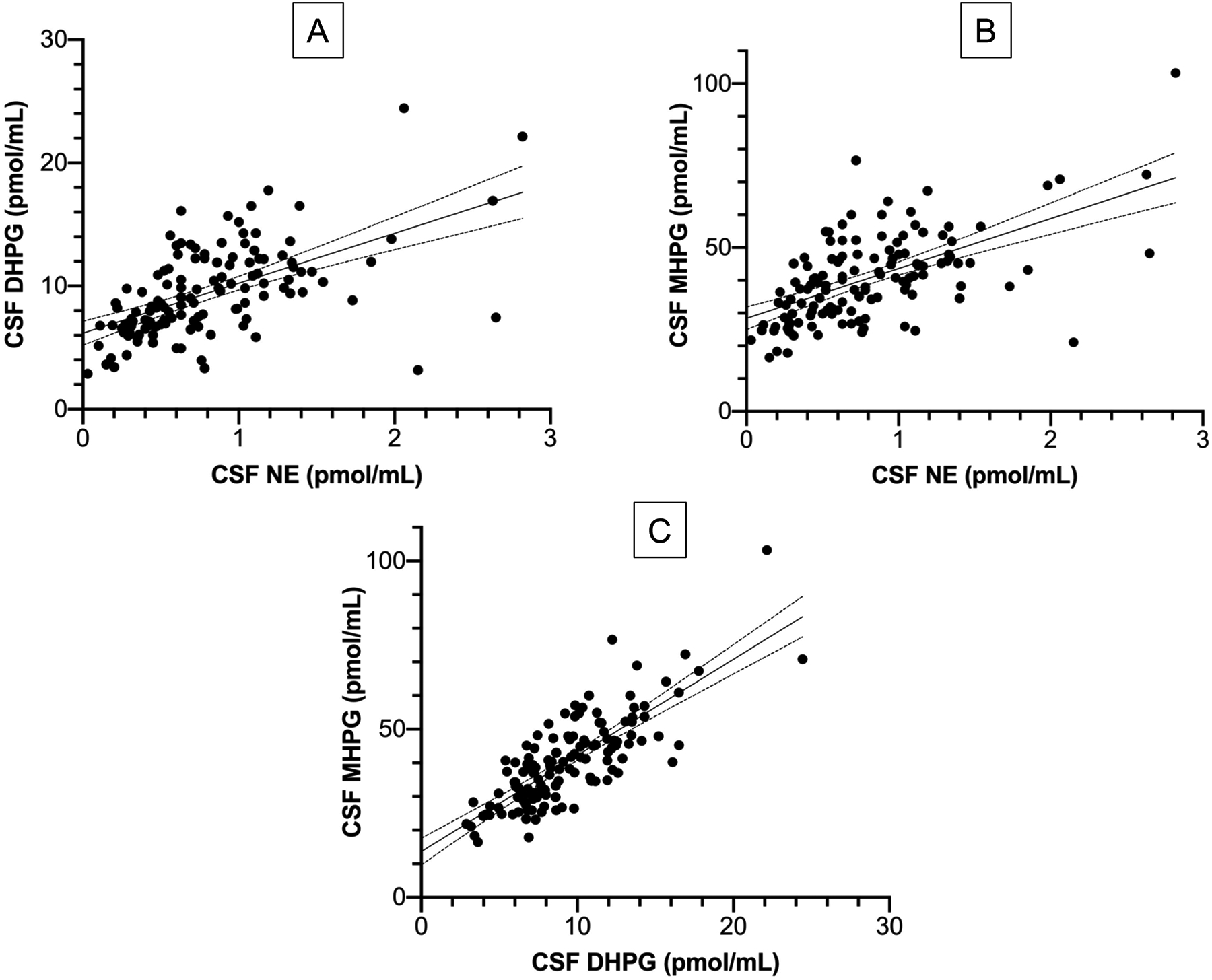
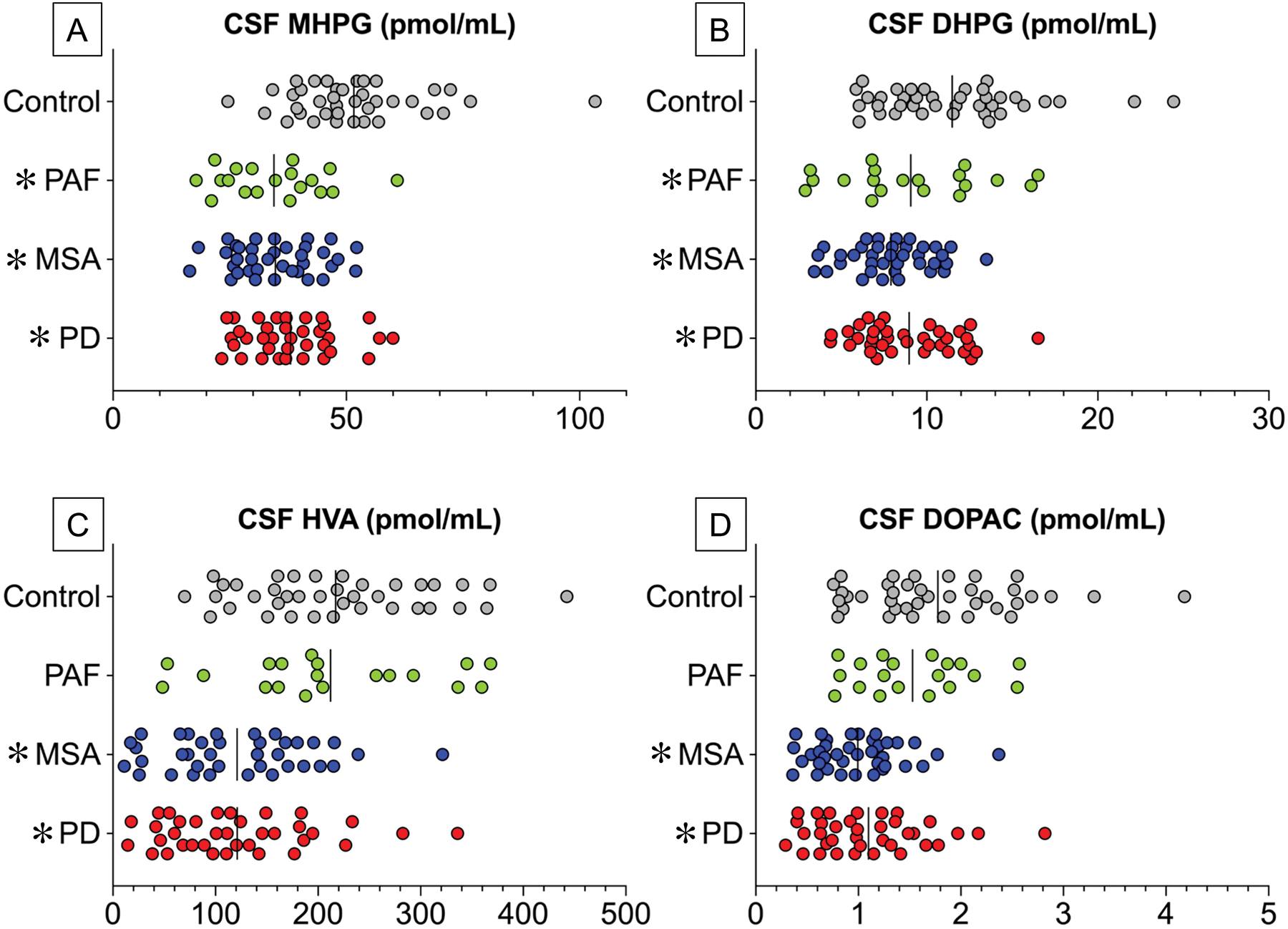
The synucleinopathies Parkinson's disease (PD), multiple system atrophy (MSA), and pure autonomic failure (PAF) are characterized by intra-cytoplasmic deposition of the protein alpha-synuclein and by catecholamine depletion. PAF, which manifests with neurogenic orthostatic hypotension (nOH) and no motor signs of central neurodegeneration, can evolve into PD+nOH. The cerebrospinal fluid (CSF) levels of catecholamine metabolites may indicate central catecholamine deficiency in these synucleinopathies, but the literature is inconsistent and incomplete. In this retrospective cohort study we reviewed data about CSF catecholamines, the dopamine metabolites 3,4-dihydroxyphenylacetic acid (DOPAC) and homovanillic acid (HVA), and the norepinephrine metabolites 3,4-dihydroxyphenylglycol (DHPG) and 3-methoxy-4-hydroxyphenylglycol (MHPG). The compounds were measured in 36 patients with PD, 37 patients with MSA, and 19 patients with PAF and in 38 controls. Compared to the control group, the PD, MSA, and PAF groups had decreased CSF MHPG (p < .0001 each by Dunnett's post hoc test), DHPG (p = .004; p < .0001; p < .0001) and norepinephrine (p = .017; p = .0003; p = .044). CSF HVA and DOPAC were decreased in PD (p < .0001 each) and MSA (p < .0001 each) but not in PAF. The three synucleinopathies therefore have in common in vivo evidence of central noradrenergic deficiency but differ in the extents of central dopaminergic deficiency-prominent in PD and MSA, less apparent in PAF. Data from putamen F-DOPA and cardiac F-dopamine neuroimaging in the same patients, post-mortem tissue catecholamines in largely separate cohorts, and review of the neuropathology literature fit with these distinctions. The results suggest a 'norepinephrine first' ascending pathogenetic sequence in synucleinopathies, with degeneration of pontine locus ceruleus noradrenergic neurons preceding the loss of midbrain substantia nigra dopaminergic neurons.
突触核蛋白病帕金森病(PD)、多系统萎缩(MSA)和单纯自主神经衰竭(PAF)的特征是细胞内沉积蛋白α-突触核蛋白和儿茶酚胺耗竭。PAF 表现为神经源性直立性低血压(nOH),没有中央神经退行性变的运动迹象,但可能会发展为 PD+nOH。脑脊液(CSF)儿茶酚胺代谢物水平可能表明这些突触核蛋白病中的中枢儿茶酚胺缺乏,但文献不一致且不完整。在这项回顾性队列研究中,我们回顾了 CSF 儿茶酚胺、多巴胺代谢物 3,4-二羟基苯乙酸(DOPAC)和高香草酸(HVA)以及去甲肾上腺素代谢物 3,4-二羟基苯乙二醇(DHPG)和 3-甲氧基-4-羟基苯乙二醇(MHPG)的数据。在 36 名 PD 患者、37 名 MSA 患者和 19 名 PAF 患者以及 38 名对照组中测量了这些化合物。与对照组相比,PD、MSA 和 PAF 组的 CSF MHPG 降低(Dunnett 事后检验,p<.0001 各),DHPG(p=0.004;p<.0001;p<.0001)和去甲肾上腺素(p=0.017;p=0.0003;p=0.044)。PD 和 MSA 中 CSF HVA 和 DOPAC 降低(p<.0001 各),但 PAF 中无降低。因此,这三种突触核蛋白病具有共同的中枢去甲肾上腺素能缺乏的体内证据,但中枢多巴胺能缺乏的程度不同-在 PD 和 MSA 中更为明显,在 PAF 中则不那么明显。同一患者的纹状体 F-DOPA 和心脏 F-多巴胺神经影像学数据、大量独立队列的死后组织儿茶酚胺以及神经病理学文献综述与这些差异相符。结果表明,在突触核蛋白病中存在“去甲肾上腺素优先”的上行发病序列,脑桥蓝斑核去甲肾上腺素能神经元变性先于中脑黑质多巴胺能神经元丧失。