Sas David J, Enders Felicity T, Gunderson Tina M, Mehta Ramila A, Olson Julie B, Seide Barbara M, Banks Carly J, Dehmel Bastian, Pellikka Patricia A, Lieske John C, Milliner Dawn S
Division of Pediatric Nephrology and Hypertension, Mayo Clinic, Rochester, MN, United States.
Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN, United States.
Front Med (Lausanne). 2021 Apr 9;8:592357. doi: 10.3389/fmed.2021.592357. eCollection 2021.
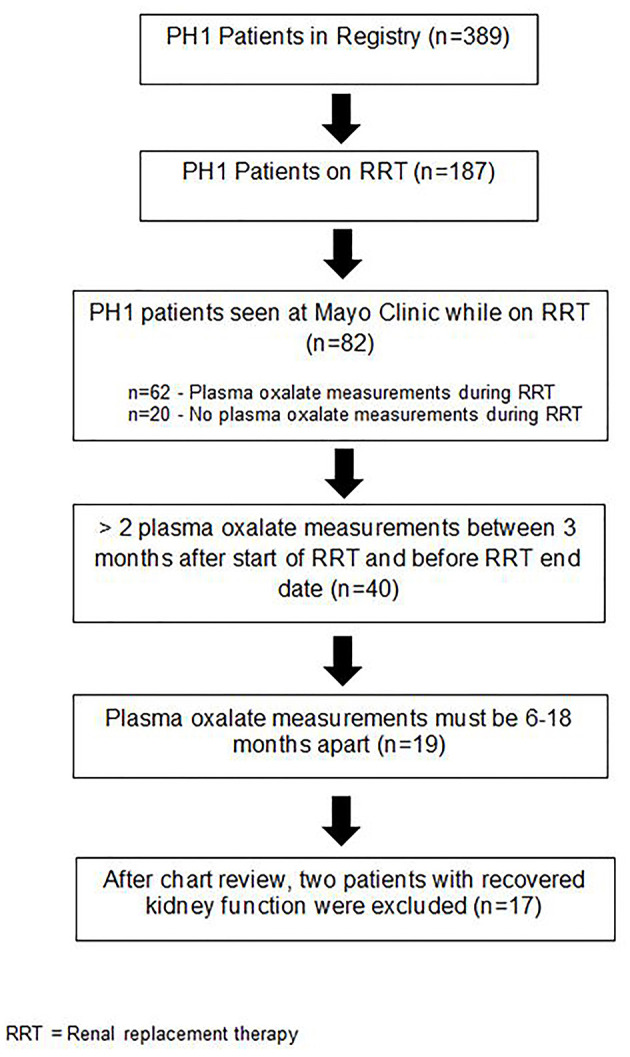
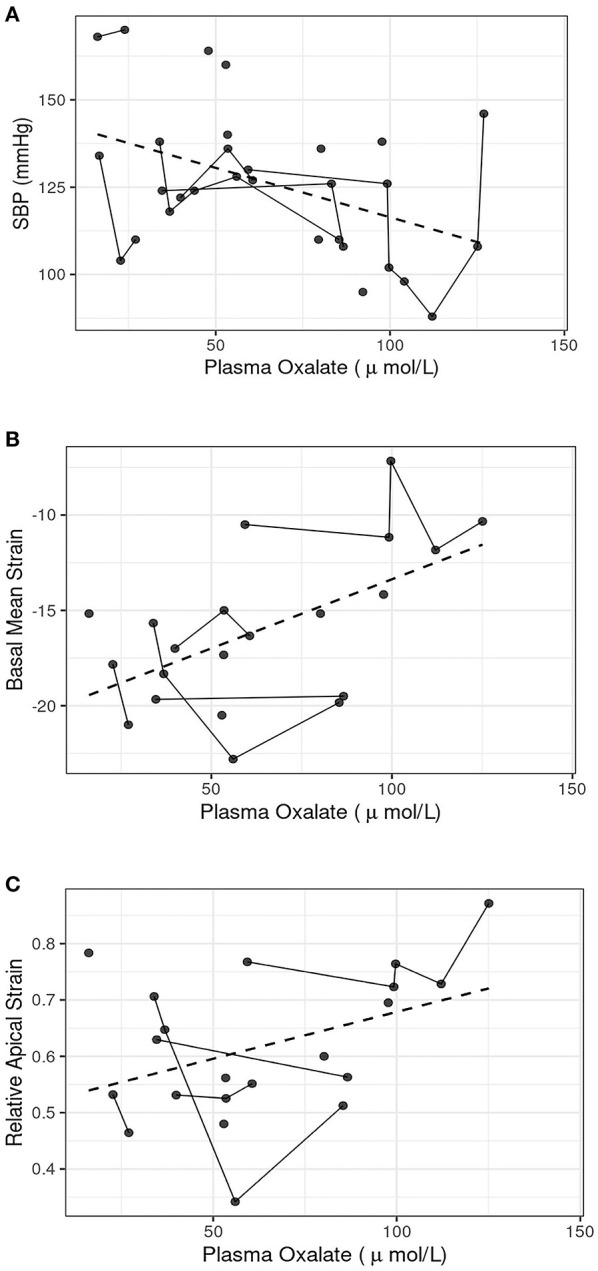
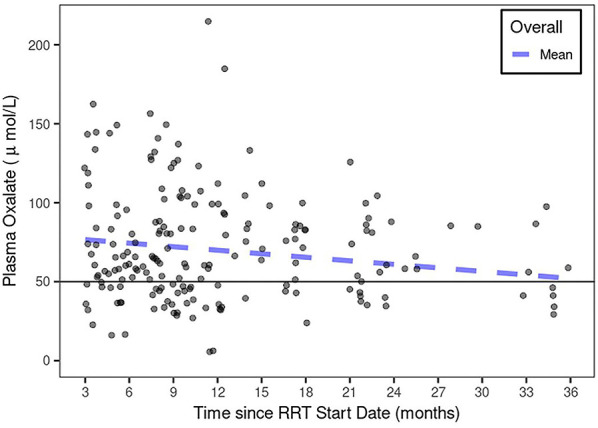
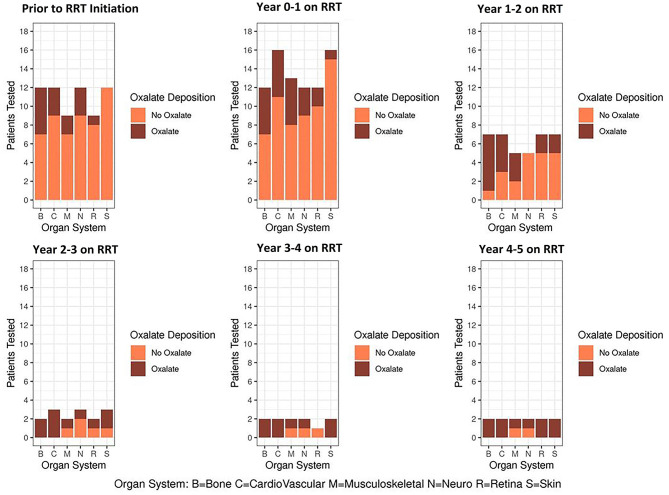
Primary hyperoxaluria type 1 (PH1) is a rare monogenic disorder characterized by excessive hepatic production of oxalate leading to recurrent nephrolithiasis, nephrocalcinosis, and progressive kidney damage, often requiring renal replacement therapy (RRT). Though systemic oxalate deposition is well-known, the natural history of PH1 during RRT has not been systematically described. In this study, we describe the clinical, laboratory, and echocardiographic features of a cohort of PH1 patients on RRT. Patients with PH1 enrolled in the Rare Kidney Stone Consortium PH Registry who progressed to require RRT, had ≥2 plasma oxalate (pOx) measurements 3-36 months after start of RRT, and at least one pair of pOx measurements between 6 and 18 months apart were retrospectively analyzed. Clinical, echocardiographic, and laboratory results were obtained from the Registry. The 17 PH1 patients in our cohort had a mean total HD hours/week of 17.4 (SD 7.9; range 7.5-36) and a range of age of RRT start of 0.2-75.9 years. The average change in plasma oxalate (pOx) over time on RRT was -0.74 [-2.9, 1.4] μmol/L/month with the mean pOx never declining below 50 μmol/L. Over time on RRT, oxalosis progressively developed in multiple organ systems. Echocardiography performed on 13 subjects showed worsening of left ventricular global longitudinal strain correlated with pOx ( < 0.05). Even when a cohort of PH1 patients were treated with intensified RRT, their predialysis pOx remained above target and they developed increasing evidence of oxalosis. Echocardiographic data suggest that cardiac dysfunction could be related to elevated pOx and may worsen over time.
1型原发性高草酸尿症(PH1)是一种罕见的单基因疾病,其特征是肝脏过度产生草酸盐,导致复发性肾结石、肾钙质沉着症和进行性肾损伤,通常需要肾脏替代治疗(RRT)。尽管全身性草酸盐沉积众所周知,但PH1在肾脏替代治疗期间的自然病史尚未得到系统描述。在本研究中,我们描述了一组接受肾脏替代治疗的PH1患者的临床、实验室和超声心动图特征。纳入罕见肾结石联盟PH注册研究的PH1患者,在开始肾脏替代治疗后3至36个月有≥2次血浆草酸盐(pOx)测量值,且至少有一对pOx测量值间隔6至18个月,对这些患者进行了回顾性分析。临床、超声心动图和实验室结果均来自该注册研究。我们队列中的17例PH1患者每周平均总血液透析时长为17.4小时(标准差7.9;范围7.5 - 36),开始肾脏替代治疗的年龄范围为0.2至75.9岁。在肾脏替代治疗期间,血浆草酸盐(pOx)随时间的平均变化为 -0.74 [-2.9, 1.4] μmol/L/月,平均pOx从未降至50 μmol/L以下。随着肾脏替代治疗时间的推移,多个器官系统逐渐出现草酸中毒。对13名受试者进行的超声心动图检查显示,左心室整体纵向应变恶化与pOx相关(<0.05)。即使一组PH1患者接受强化肾脏替代治疗,其透析前pOx仍高于目标值,且草酸中毒的证据越来越多。超声心动图数据表明,心脏功能障碍可能与pOx升高有关,且可能随时间恶化。