Veterans Affairs Boston Healthcare System West Roxbury MA.
Brigham and Women's Hospital Boston MA.
J Am Heart Assoc. 2021 May 4;10(9):e018481. doi: 10.1161/JAHA.120.018481. Epub 2021 Apr 26.
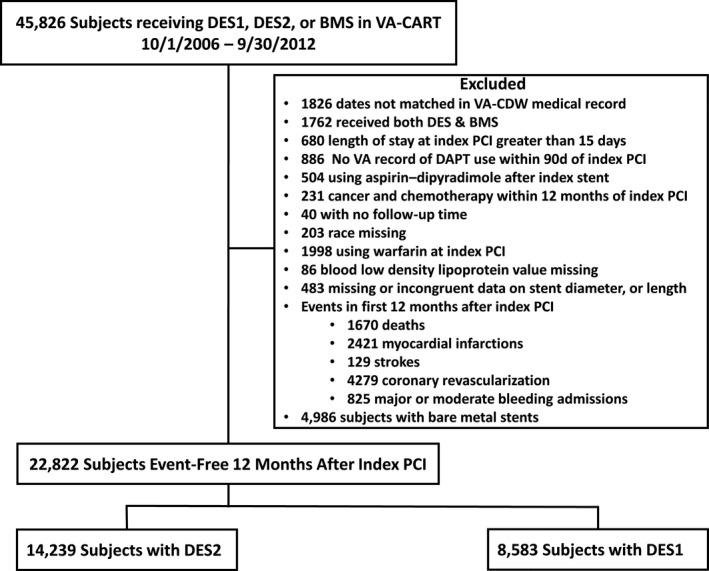
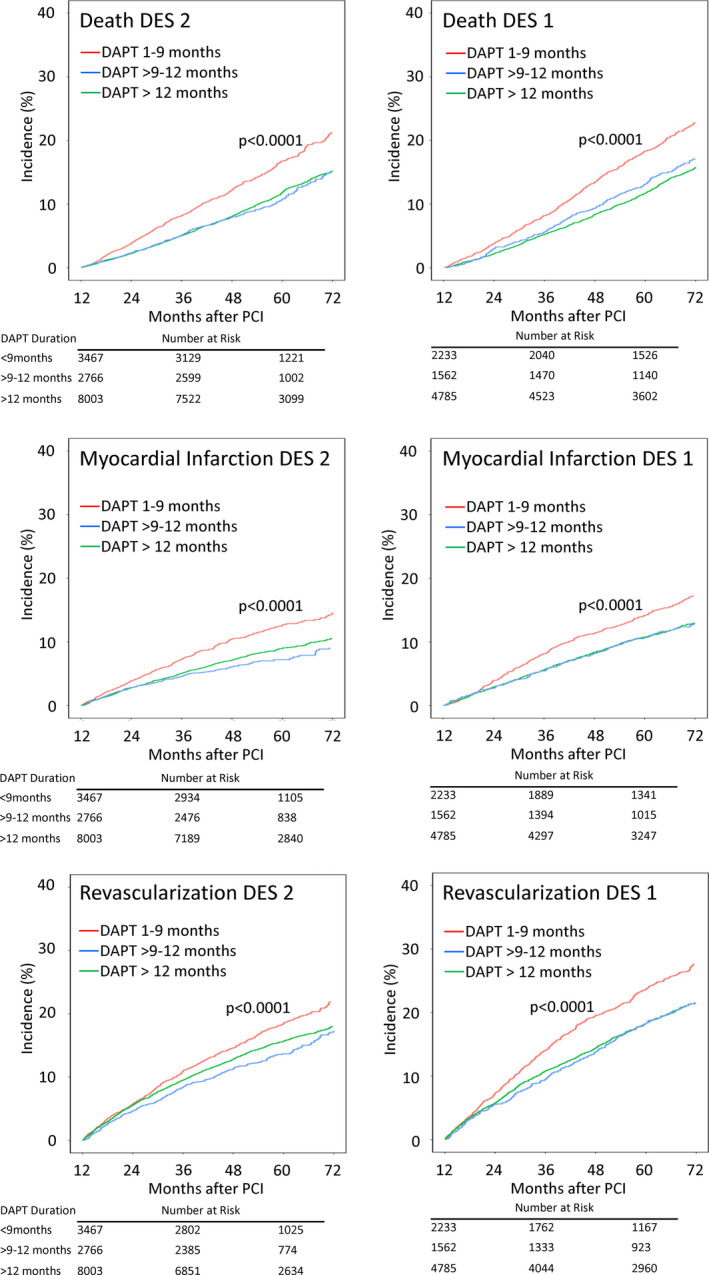
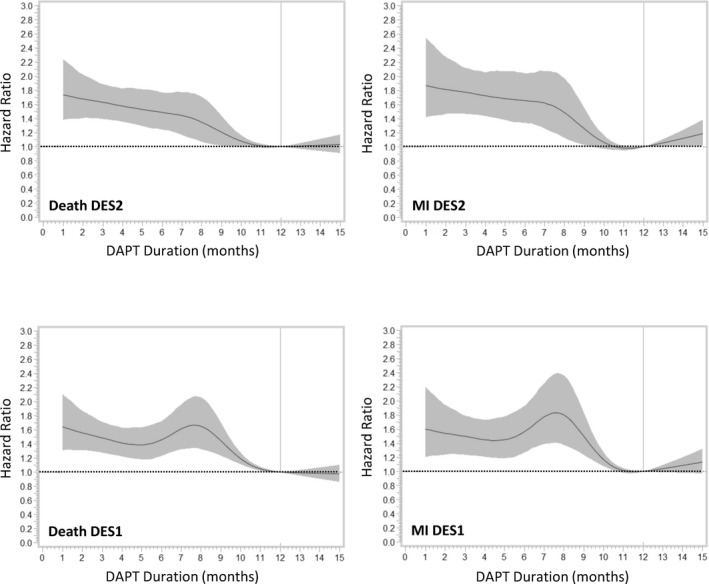
Background Premature discontinuation of dual antiplatelet therapy (DAPT) after percutaneous coronary intervention is related to higher short-term risks of adverse outcomes. Whether these risks persist in the long-term is uncertain. Methods and Results We assessed all patients having percutaneous coronary intervention with coronary second- or first-generation drug-eluting stents in the Veterans Affairs healthcare system between 2006 and 2012 who were free of major ischemic or bleeding events in the first 12 months. The characteristics of patients who stopped DAPT prematurely (1-9 months duration), compared with >9 to 12 months, or extended duration (>12 months) were assessed by odds ratios (ORs) from multivariable logistic models. The risk of adverse clinical outcomes over a mean 5.1 years in patients who stopped DAPT prematurely was assessed by hazard ratios (HRs) and 95% CIs from Cox regression models. A total of 14 239 had second-generation drug-eluting stents, and 8583 had first-generation drug-eluting stents. Premature discontinuation of DAPT was more likely in Black patients (OR, 1.54; 95% CI, 1.40-1.68), patients with greater frailty (OR, 1.04; 95% CI, 1.03-1.05), and patients with higher low-density lipoprotein cholesterol, and less likely in patients on statins (OR, 0.87; 95% CI, 0.80-0.95). Patients who stopped DAPT prematurely had higher long-term risks of death (second-generation drug-eluting stents: HR, 1.35; 95% CI, 1.19-1.56), myocardial infarction (second-generation drug-eluting stents: HR, 1.46; 95% CI, 1.22-1.74), and repeated coronary revascularization (second-generation drug-eluting stents: HR, 1.24; 95% CI, 1.08-1.41). Conclusions Patients who stop DAPT prematurely have features that reflect greater frailty, poorer medication use, and other social factors. They continue to have higher risks of major adverse outcomes over the long-term and may require more intensive surveillance many years after percutaneous coronary intervention.
经皮冠状动脉介入治疗(PCI)后双联抗血小板治疗(DAPT)过早停药与短期不良结局的风险增加相关。这些风险是否会持续存在尚不确定。
我们评估了 2006 年至 2012 年期间在退伍军人事务部医疗保健系统中接受 PCI 治疗的、在最初 12 个月内无重大缺血或出血事件的、使用第二代或第一代药物洗脱支架的所有患者。通过多变量逻辑模型的比值比(OR)评估与 DAPT 过早停药(1-9 个月)相比,持续时间>9-12 个月或>12 个月的患者的特征。通过 Cox 回归模型的风险比(HR)和 95%CI 评估在平均 5.1 年时 DAPT 过早停药患者的不良临床结局风险。共有 14239 名患者接受了第二代药物洗脱支架治疗,8583 名患者接受了第一代药物洗脱支架治疗。黑人患者(OR,1.54;95%CI,1.40-1.68)、身体虚弱程度更高的患者(OR,1.04;95%CI,1.03-1.05)和低密度脂蛋白胆固醇水平更高的患者更有可能过早停止 DAPT,而服用他汀类药物的患者(OR,0.87;95%CI,0.80-0.95)则不太可能过早停止 DAPT。过早停止 DAPT 的患者发生死亡(第二代药物洗脱支架:HR,1.35;95%CI,1.19-1.56)、心肌梗死(第二代药物洗脱支架:HR,1.46;95%CI,1.22-1.74)和重复冠状动脉血运重建(第二代药物洗脱支架:HR,1.24;95%CI,1.08-1.41)的长期风险更高。
过早停止 DAPT 的患者具有反映身体虚弱、药物使用不佳和其他社会因素的特征。他们在长期内仍有更高的主要不良结局风险,并且可能需要在 PCI 后多年进行更密集的监测。