Department of Hematology, Oncology, Clinical Immunology, Rheumatology, Medical School, University of Saarland, Kirrberger Str. 100, 66421, Homburg, Germany.
Institute for Medical Informatics, Statistics and Epidemiology, University Leipzig, Leipzig, Germany.
Eur J Nucl Med Mol Imaging. 2021 Oct;48(11):3550-3559. doi: 10.1007/s00259-021-05348-6. Epub 2021 Apr 29.
Fluorine-18 fluorodeoxyglucose positron emission tomography combined with computed tomography (FDG PET/CT) is the standard for staging aggressive non-Hodgkin lymphoma (NHL). Limited data from prospective studies is available to determine whether initial staging by FDG PET/CT provides treatment-relevant information of bone marrow (BM) involvement (BMI) and thus could spare BM biopsy (BMB).
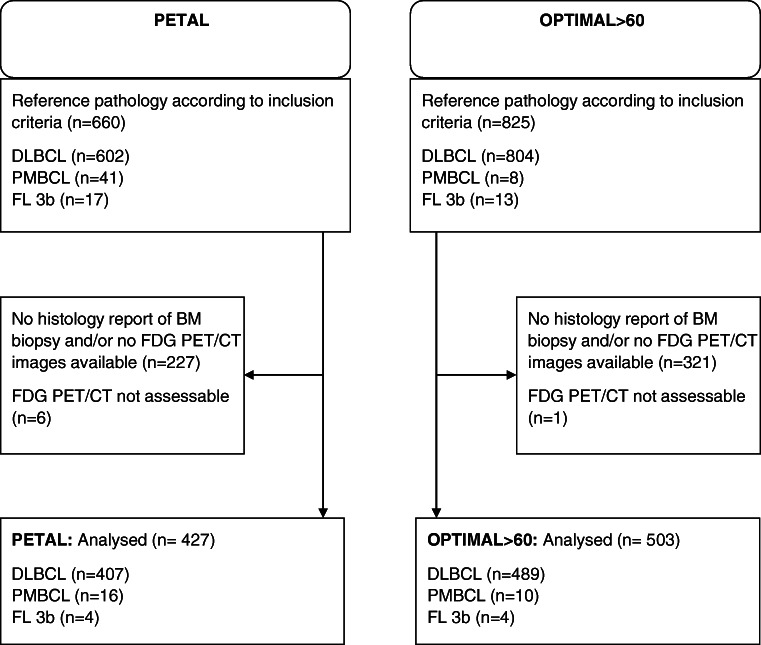
Patients from PETAL (NCT00554164) and OPTIMAL>60 (NCT01478542) with aggressive B-cell NHL initially staged by FDG PET/CT and BMB were included in this pooled analysis. The reference standard to confirm BMI included a positive BMB and/or FDG PET/CT confirmed by targeted biopsy, complementary imaging (CT or magnetic resonance imaging), or concurrent disappearance of focal FDG-avid BM lesions with other lymphoma manifestations during immunochemotherapy.
Among 930 patients, BMI was detected by BMB in 85 (prevalence 9%) and by FDG PET/CT in 185 (20%) cases, for a total of 221 cases (24%). All 185 PET-positive cases were true positive, and 709 of 745 PET-negative cases were true negative. For BMB and FDG PET/CT, sensitivity was 38% (95% confidence interval [CI]: 32-45%) and 84% (CI: 78-88%), specificity 100% (CI: 99-100%) and 100% (CI: 99-100%), positive predictive value 100% (CI: 96-100%) and 100% (CI: 98-100%), and negative predictive value 84% (CI: 81-86%) and 95% (CI: 93-97%), respectively. In all of the 36 PET-negative cases with confirmed BMI patients had other adverse factors according to IPI that precluded a change of standard treatment. Thus, the BMB would not have influenced the patient management.
In patients with aggressive B-cell NHL, routine BMB provides no critical staging information compared to FDG PET/CT and could therefore be omitted.
NCT00554164 and NCT01478542.
氟-18 氟代脱氧葡萄糖正电子发射断层扫描(FDG PET/CT)与计算机断层扫描(CT)结合是侵袭性非霍奇金淋巴瘤(NHL)分期的标准。目前仅有少量前瞻性研究的数据可用于确定 FDG PET/CT 初始分期是否提供与治疗相关的骨髓(BM)受累(BMI)信息,从而是否可以避免骨髓活检(BMB)。
本研究纳入了来自 PETAL(NCT00554164)和 OPTIMAL>60(NCT01478542)的侵袭性 B 细胞 NHL 患者,这些患者最初通过 FDG PET/CT 和 BMB 进行分期。确认 BMI 的参考标准包括阳性 BMB 和/或 FDG PET/CT 通过靶向活检、补充成像(CT 或磁共振成像)或在免疫化学治疗期间与其他淋巴瘤表现同时消失的局灶性 FDG 摄取 BM 病变得到确认。
在 930 例患者中,BMB 检测到 BMI 为 85 例(患病率为 9%),FDG PET/CT 检测到 BMI 为 185 例(20%),共 221 例(24%)。所有 185 例 PET 阳性病例均为真阳性,745 例 PET 阴性病例均为真阴性。BMB 和 FDG PET/CT 的敏感性分别为 38%(95%置信区间[CI]:32-45%)和 84%(CI:78-88%),特异性为 100%(CI:99-100%)和 100%(CI:99-100%),阳性预测值为 100%(CI:96-100%)和 100%(CI:98-100%),阴性预测值为 84%(CI:81-86%)和 95%(CI:93-97%)。在所有 36 例 PET 阴性且证实有 BMI 的患者中,根据国际预后指数(IPI)存在其他不良因素,排除了标准治疗的改变。因此,BMB 不会影响患者的管理。
在侵袭性 B 细胞 NHL 患者中,与 FDG PET/CT 相比,常规 BMB 并未提供关键的分期信息,因此可以省略。
NCT00554164 和 NCT01478542。