Department of Anesthesiology, CUB Erasme, Université Libre de Bruxelles, 808 route de Lennik, 1070, Bruxelles, Belgium.
Department of Anesthesiology and Intensive Care, Hôpitaux Universitaires Paris-Sud, Université Paris-Sud, Paul Brousse Hospital, Assistance Publique Hôpitaux de Paris (APHP), Université Paris-Saclay, 12 Avenue Paul Vaillant Couturier, 94800, Villejuif, France.
BMC Anesthesiol. 2021 Apr 30;21(1):135. doi: 10.1186/s12871-021-01353-2.
The potential relationship between a mild acute kidney injury (AKI) observed in the immediate postoperative period after major surgery and its effect on long term renal function remains poorly defined. According to the "Kidney Disease: Improving Global Outcomes" (KDIGO) classification, a mild injury corresponds to a KIDIGO stage 1, characterized by an increase in creatinine of at least 0.3 mg/dl within a 48-h window or 1.5 to 1.9 times the baseline level within the first week post-surgery. We tested the hypothesis that patients who underwent intermediate-to high-risk abdominal surgery and developed mild AKI in the following days would be at an increased risk of long-term renal injury compared to patients with no postoperative AKI.
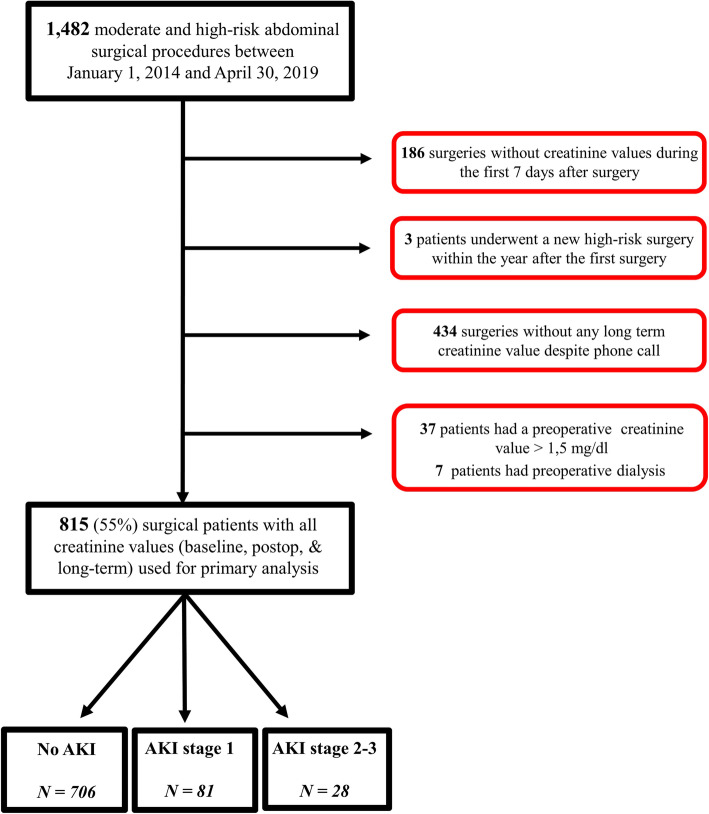
All consecutive adult patients with a plasma creatinine value ≤1.5 mg/dl who underwent intermediate-to high-risk abdominal surgery between 2014 and 2019 and who had at least three recorded creatinine measurements (before surgery, during the first seven postoperative days, and at long-term follow up [6 months-2 years]) were included. AKI was defined using a "modified" (without urine output criteria) KDIGO classification as mild (stage 1 characterised by an increase in creatinine of > 0.3 mg/dl within 48-h or 1.5-1.9 times baseline) or moderate-to-severe (stage 2-3 characterised by increase in creatinine 2 to 3 times baseline or to ≥4.0 mg/dl). The exposure (postoperative kidney injury) and outcome (long-term renal injury) were defined and staged according to the same KDIGO initiative criteria. Development of long-term renal injury was compared in patients with and without postoperative AKI.
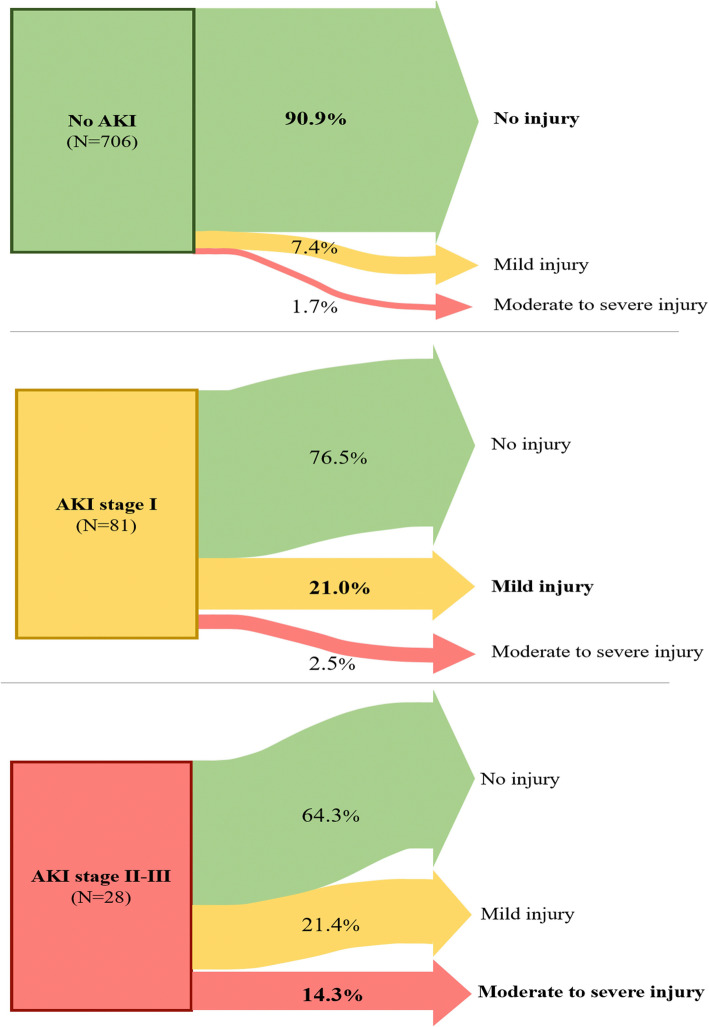
Among the 815 patients included, 109 (13%) had postoperative AKI (81 mild and 28 moderate-to-severe). The median long-term follow-up was 360, 354 and 353 days for the three groups respectively (P = 0.2). Patients who developed mild AKI had a higher risk of long-term renal injury than those who did not (odds ratio 3.1 [95%CI 1.7-5.5]; p < 0.001). In multivariable analysis, mild postoperative AKI was independently associated with an increased risk of developing long-term renal injury (adjusted odds ratio 4.5 [95%CI 1.8-11.4]; p = 0.002).
Mild AKI after intermediate-to high-risk abdominal surgery is associated with a higher risk of long-term renal injury 1 y after surgery.
在大手术后的即刻术后期间观察到的轻度急性肾损伤(AKI)与其对长期肾功能的影响之间的潜在关系仍未得到明确界定。根据“肾脏病:改善全球结局”(KDIGO)分类,轻度损伤对应于 KDIGO 分期 1,其特征是在 48 小时窗口内肌酐升高至少 0.3mg/dl,或在手术后第一周内升高至基线水平的 1.5 至 1.9 倍。我们检验了这样一个假设,即接受中高危腹部手术并在接下来几天内发生轻度 AKI 的患者与无术后 AKI 的患者相比,长期肾功能损伤的风险增加。
所有在 2014 年至 2019 年间接受中高危腹部手术且血浆肌酐值≤1.5mg/dl 的连续成年患者,至少有三次记录的肌酐测量值(术前、术后前 7 天和长期随访[6 个月-2 年])均纳入研究。AKI 采用“改良”(无尿输出标准)KDIGO 分类定义为轻度(第 1 期,特征为肌酐在 48 小时内升高>0.3mg/dl,或升高至基线的 1.5-1.9 倍)或中重度(第 2-3 期,特征为肌酐升高 2-3 倍基线或升高至≥4.0mg/dl)。根据相同的 KDIGO 倡议标准定义暴露(术后肾脏损伤)和结局(长期肾脏损伤)。比较术后 AKI 患者和无术后 AKI 患者的长期肾损伤发生情况。
在纳入的 815 例患者中,109 例(13%)发生术后 AKI(81 例轻度,28 例中重度)。三组患者的中位长期随访时间分别为 360、354 和 353 天(P=0.2)。与未发生 AKI 的患者相比,发生轻度 AKI 的患者发生长期肾损伤的风险更高(比值比 3.1[95%CI 1.7-5.5];p<0.001)。多变量分析显示,术后轻度 AKI 与发生长期肾损伤的风险增加独立相关(校正比值比 4.5[95%CI 1.8-11.4];p=0.002)。
中高危腹部手术后的轻度 AKI 与术后 1 年发生长期肾损伤的风险增加相关。