Department of Pediatric Rheumatology, Medical University Sofia, Sofia, Bulgaria.
Department of Pediatric Rheumatology and Immunology, University Hospital Münster, Albert-Schweitzer-Campus 1, Building D3, D-48149, Muenster, Germany.
Pediatr Rheumatol Online J. 2021 May 1;19(1):64. doi: 10.1186/s12969-021-00553-x.
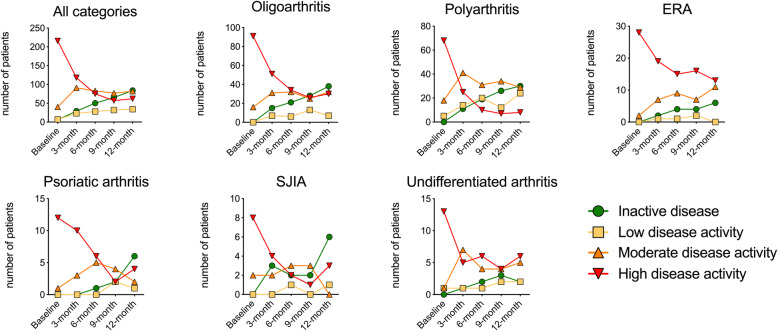
Juvenile idiopathic arthritis (JIA) is a heterogeneous group of inflammatory joint disorders with a chronic-remitting disease course. Treat-to-target approaches have been proposed but monitoring disease activity and predicting the response to treatment remains challenging.
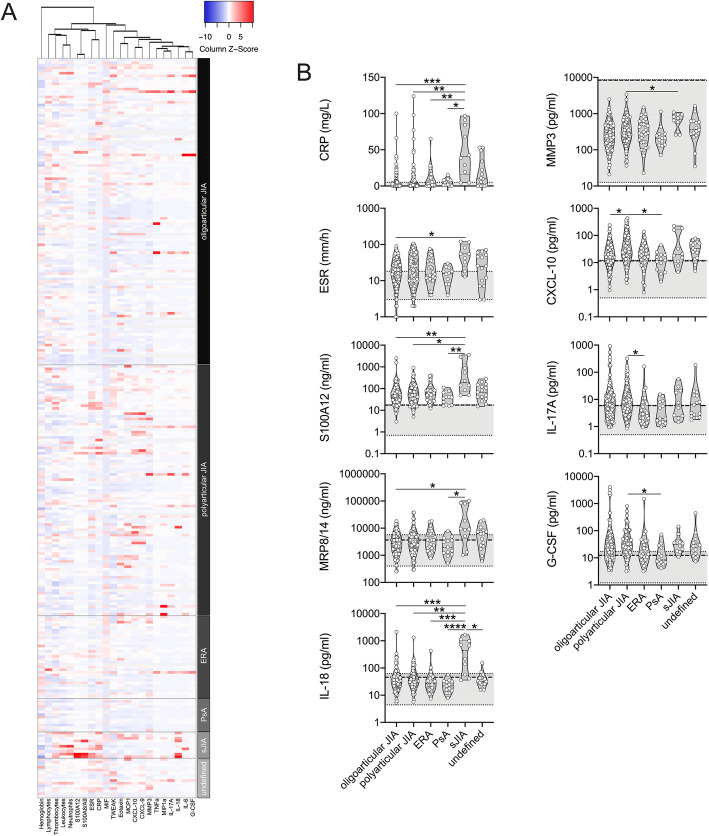
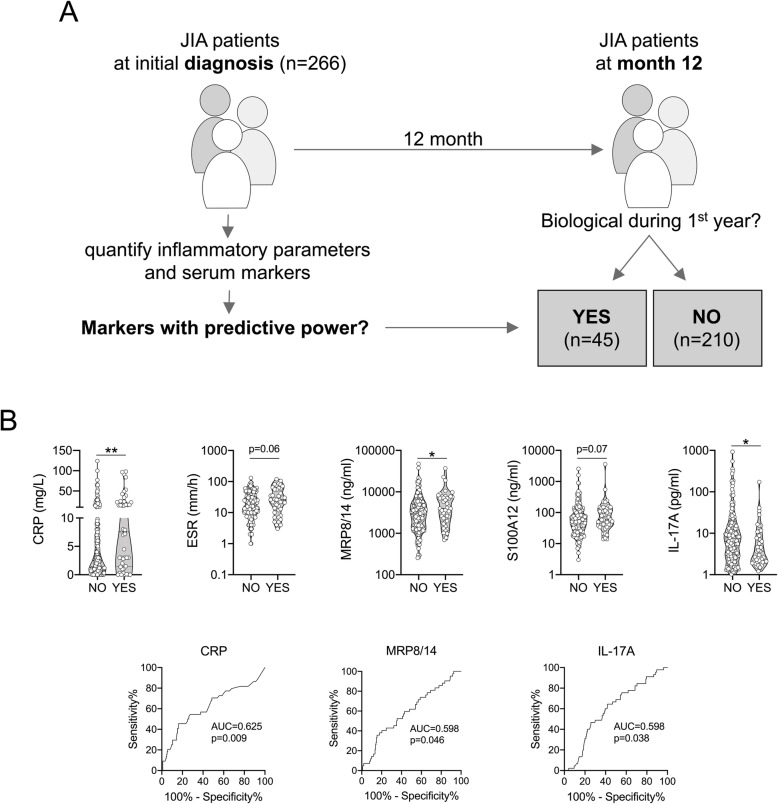
We analyzed biomarkers and their relationship to outcome within the first year after JIA diagnosis in the German Inception Cohort of Newly diagnosed patients with JIA (ICON-JIA). CRP, CXCL9, CXCL10, CXCL11, erythrocyte sedimentation rate, G-CSF, IL-6, IL-17A, IL-18, MCP-1, MIP-1α, MMP-3, S100A8/A9, S100A12, TNFα, and TWEAK were measured at baseline and 3 months later.
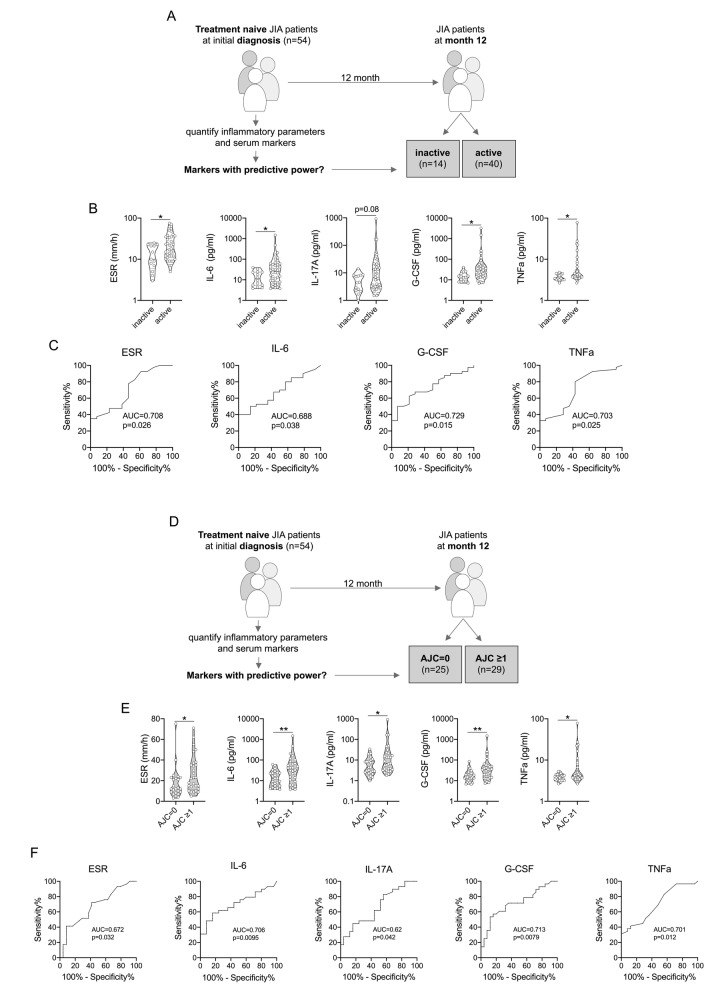
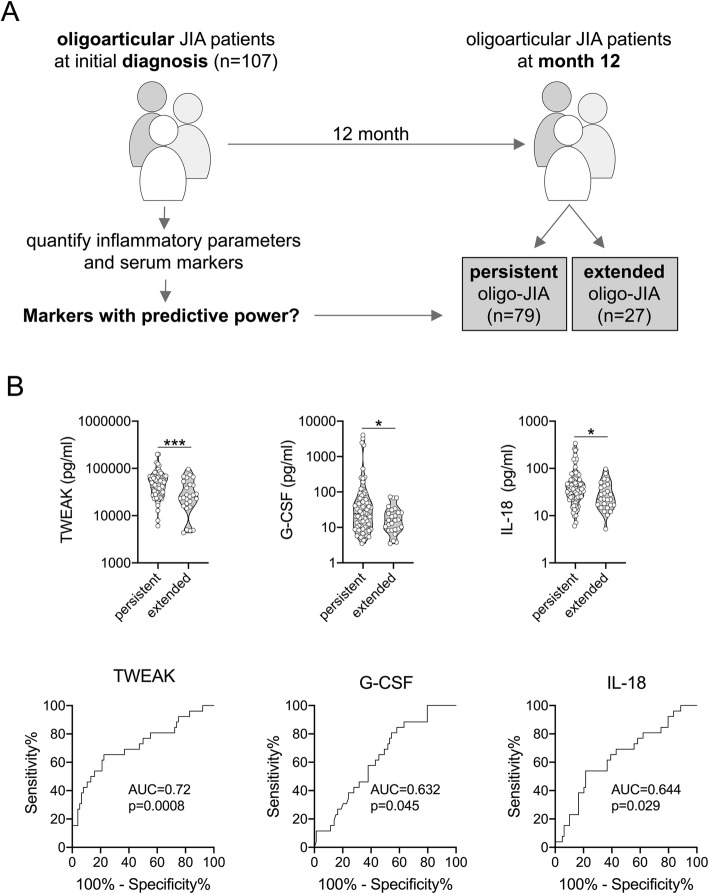
Two-hundred-sixty-six JIA patients with active disease at baseline were included, with oligoarthritis and rheumatoid factor-negative polyarthritis representing the most frequent categories (72.9%). Most biomarkers were elevated in JIA compared to healthy pediatric controls. Patients with systemic JIA had higher CRP, S100A8/A9 and S100A12 levels compared to other JIA categories. Baseline levels of TWEAK, G-CSF and IL-18 were lower in oligoarthritis patients with disease extension within 1 year. Increased baseline levels of CRP, S100A8/A9, S100A12 and ESR were associated with the subsequent addition of biologic disease-modifying antirheumatic drugs (DMARDs). Higher baseline ESR, G-CSF, IL-6, IL-17A and TNF levels indicated an increased risk for ongoing disease activity after 12 months.
Our data demonstrate that elevated baseline levels of CRP, S100A8/A9 and S100A12 as well as increased ESR are associated with the necessity to escalate therapy during the first 12 month of follow-up. Furthermore, biomarkers related to Th17 activation may inform on future disease course in previously treatment-naïve JIA patients.
幼年特发性关节炎(JIA)是一组异质性的炎症性关节疾病,具有慢性缓解病程。已经提出了针对目标的治疗方法,但监测疾病活动和预测治疗反应仍然具有挑战性。
我们在德国新诊断的幼年特发性关节炎患者的起始队列(ICON-JIA)中分析了 JIA 诊断后第一年的生物标志物及其与结局的关系。在基线和 3 个月时测量 CRP、CXCL9、CXCL10、CXCL11、红细胞沉降率、G-CSF、IL-6、IL-17A、IL-18、MCP-1、MIP-1α、MMP-3、S100A8/A9、S100A12、TNFα 和 TWEAK。
共纳入 266 例基线时疾病活动的 JIA 患者,最常见的类别为寡关节炎和类风湿因子阴性多关节炎(72.9%)。与健康儿科对照组相比,JIA 患者的大多数生物标志物升高。与其他 JIA 类别相比,全身型 JIA 患者的 CRP、S100A8/A9 和 S100A12 水平更高。在 1 年内疾病扩展的寡关节炎患者中,基线时 TWEAK、G-CSF 和 IL-18 水平较低。CRP、S100A8/A9、S100A12 和 ESR 的基线水平升高与随后添加生物性疾病修饰抗风湿药物(DMARDs)有关。较高的基线 ESR、G-CSF、IL-6、IL-17A 和 TNF 水平表明在 12 个月后疾病活动持续存在的风险增加。
我们的数据表明,CRP、S100A8/A9 和 S100A12 的基线水平升高以及 ESR 增加与在随访的前 12 个月中需要升级治疗有关。此外,与 Th17 激活相关的生物标志物可能提示以前未经治疗的 JIA 患者的未来疾病进程。