Shen Hongzhang, Xiong Kangwei, Wu Xiangyu, Cheng Sile, Lou Qifeng, Jin Hangbin, Zhang Xiaofeng
Department of Gastroenterology, Affiliated Hangzhou First People's Hospital, Zhejiang University School of Medicine, Hangzhou, China.
Department of Gastroenterology, The Second Hospital of Anhui Medical University, Hefei, China.
Gastroenterol Res Pract. 2021 Apr 12;2021:6894248. doi: 10.1155/2021/6894248. eCollection 2021.
To evaluate the diagnostic value of gastrin-17 (G-17) and pepsinogen (PG) in gastric cancer (GC) screening in China, especially eastern China, and to determine the best diagnostic combination and threshold (cutoff values) to screen out patients who need gastroscopy.
The serum concentrations of G-17 and pepsinogen I and II (PGI and PGII) in 834 patients were analyzed, and the PGI/PGII ratio (PGR) was calculated. According to pathological results, patients can be divided into chronic nonatrophic gastritis (NAG)/chronic atrophic gastritis (CAG)/intraepithelial neoplasia (IN)/GC groups. The differences in G-17, PG, and PGR in each group were analyzed, and their values in GC diagnosis were evaluated separately and in combination.
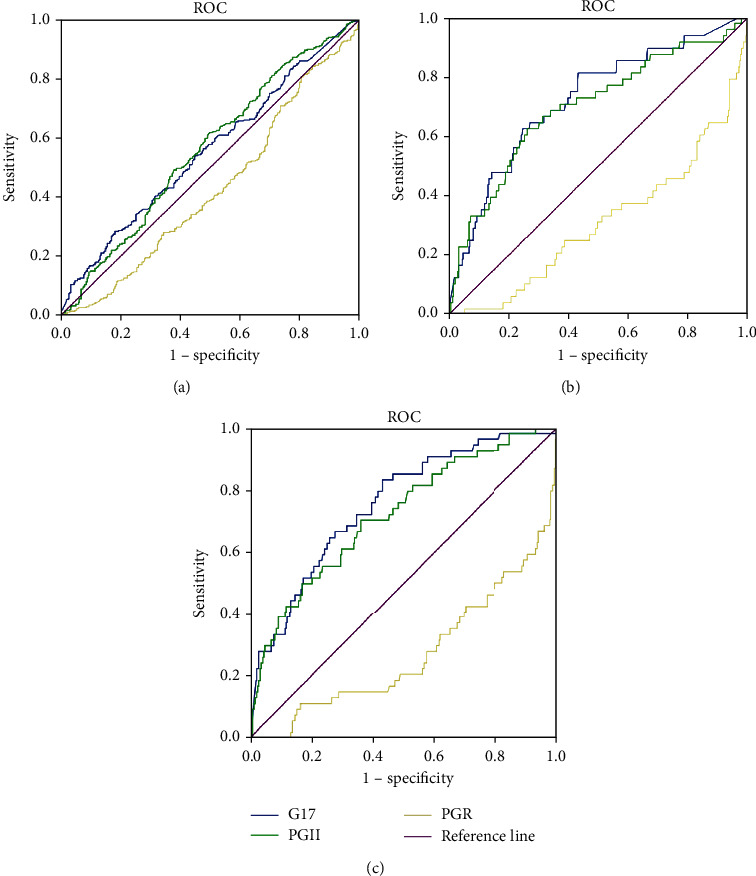
There were differences in serum G-17, PGII, and PGR among the four groups (NAG/CAG/IN/GC) ( ≤ 0.001). In total, 54 GC cases were diagnosed, of which 50% were early GC. There was no significant difference in the PGI levels among the four groups ( = 0.377). NAG and CAG composed the chronic gastritis (CG) group. The G-17 and PGII levels in the IN and GC groups were higher than those in the CG group (both ≤ oth ), while the PGR levels were lower ( ≤ lower). When distinguishing NAG from CAG, the best cutoff value for G-17 was 9.25 pmol/L, PGII was 7.06 g/L, and PGR was 12.07. When distinguishing CG from IN, the best cutoff value for G-17 was 3.86 pmol/L, PGII was 11.92 g/L, and PGR was 8.26. When distinguishing CG from GC, the best cutoff value for G-17 was 3.89 pmol/L, PGII was 9.16 g/L, and PGR was 14.14. The sensitivity, specificity, accuracy, and positive and negative predictive values of G-17/PGII/PGR for GC diagnosis were 83.3%/70.4%/79.6%, 51.8%/56.3%/47.8%, 53.8%/57.2%/49.9%, 10.7%/10.9%/9.6%, and 97.8%/96.5%/97.1%, respectively. The sensitivity, specificity, accuracy, and positive predictive and negative predictive values of PGII/G-17 vs. PGR/G-17 vs. PGR/PGII in the diagnosis of GC were 63.0% vs. 70.4% vs. 64.8%, 70.5% vs. 70.1% vs. 60.4%, 70.0% vs. 70.1% vs. 60.7%, 12.9% vs. 14.0% vs. 10.2%, and 96.5% vs. 97.2% vs. 96.1%, respectively.
The PGII and G-17 levels in patients with gastric IN and GC were significantly increased, while the serum PGR level was significantly decreased. Serological detection is effective for screening GC. The combination of different markers can improve the diagnostic efficiency. The highest diagnostic accuracy was G-17 combined with PGR, and the best cutoff values were G - 17 > 3.89 pmol/L and PGR < 14.14.
评估胃泌素-17(G-17)和胃蛋白酶原(PG)在中国尤其是中国东部地区胃癌(GC)筛查中的诊断价值,并确定筛选出需要进行胃镜检查患者的最佳诊断组合及阈值(临界值)。
分析834例患者血清中G-17、胃蛋白酶原I和II(PGI和PGII)的浓度,并计算PGI/PGII比值(PGR)。根据病理结果,患者可分为慢性非萎缩性胃炎(NAG)/慢性萎缩性胃炎(CAG)/上皮内瘤变(IN)/GC组。分析每组中G-17、PG和PGR的差异,并分别及联合评估它们在GC诊断中的价值。
四组(NAG/CAG/IN/GC)之间血清G-17、PGII和PGR存在差异(P≤0.001)。共诊断出54例GC病例,其中50%为早期GC。四组间PGI水平无显著差异(P = 0.377)。NAG和CAG组成慢性胃炎(CG)组。IN组和GC组的G-17和PGII水平高于CG组(均P≤oth),而PGR水平较低(P≤lower)。区分NAG与CAG时,G-17的最佳临界值为9.25 pmol/L,PGII为7.06 μg/L,PGR为12.07。区分CG与IN时,G-17的最佳临界值为3.86 pmol/L,PGII为11.92 μg/L,PGR为8.26。区分CG与GC时,G-17的最佳临界值为3.89 pmol/L,PGII为9.16 μg/L,PGR为14.14。G-17/PGII/PGR对GC诊断的敏感性、特异性、准确性以及阳性和阴性预测值分别为83.3%/70.4%/79.6%、51.8%/56.3%/47.8%、53.8%/57.2%/49.9%、10.7%/10.9%/9.6%以及97.8%/96.5%/97.1%。PGII/G-17、PGR/G-17、PGR/PGII在GC诊断中的敏感性、特异性、准确性以及阳性预测值和阴性预测值分别为63.0%、70.4%、64.8%;70.5%、70.1%、60.4%;70.0%、70.1%、60.7%;12.9%、14.0%、10.2%;96.5%、97.2%、96.1%。
胃IN和GC患者的PGII和G-17水平显著升高,而血清PGR水平显著降低。血清学检测对GC筛查有效。不同标志物联合可提高诊断效率。诊断准确性最高的是G-17与PGR联合,最佳临界值为G-17>3.89 pmol/L且PGR<14.14。