Division of Medical Oncology, National Cancer Centre Singapore, Singapore.
Division of Clinical Trials and Epidemiological Sciences, National Cancer Centre Singapore, Singapore.
Cancer Rep (Hoboken). 2021 Oct;4(5):e1393. doi: 10.1002/cnr2.1393. Epub 2021 May 3.
Pancreatic adenocarcinoma (PDAC) is highly lethal. Surgery offers the only chance of cure, but 5-year overall survival (OS) after surgical resection and adjuvant therapy remains dismal. Adjuvant trials were mostly conducted in the West enrolling fit patients. Applicability to a general population, especially Asia has not been described adequately.
We aimed to evaluate the clinical outcomes, prognostic factors of survival, pattern, and timing of recurrence after curative resection in an Asian institution.
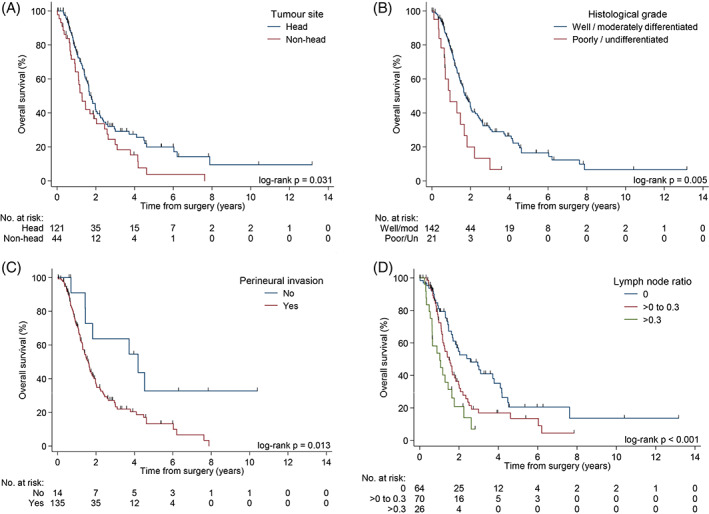
The clinicopathologic and survival outcomes of 165 PDAC patients who underwent curative resection between 1998 and 2013 were reviewed retrospectively. Median age at surgery was 62.0 years. 55.2% were male, and 73.3% had tumors involving the head of pancreas. The median OS of the entire cohort was 19.7 months. Median OS of patients who received adjuvant chemotherapy was 23.8 months. Negative predictors of survival include lymph node ratio (LNR) of >0.3 (HR = 3.36, P = .001), tumor site involving the body or tail of pancreas (HR = 1.59, P = .046), presence of perineural invasion (PNI) (HR = 2.36, P = .018) and poorly differentiated/undifferentiated tumor grade (HR = 1.86, P = .058). The median time to recurrence was 8.87 months, with 66.1% and 81.2% of patients developing recurrence at 12 months and 24 months respectively. The most common site of recurrence was the liver.
The survival of Asian patients with resected PDAC who received adjuvant chemotherapy is comparable to reported randomized trials. Clinical characteristics seem similar to Western patients. Hence, geographical locations may not be a necessary stratification factor in RCTs. Conversely, lymph node ratio and status of PNI ought to be incorporated.
胰腺导管腺癌(PDAC)的致死率很高。手术是唯一可能治愈的方法,但手术后进行辅助治疗的患者 5 年总生存率(OS)仍然很低。辅助试验主要在西方国家进行,纳入的是身体状况良好的患者。其在一般人群中的适用性,尤其是亚洲人群,尚未得到充分描述。
我们旨在评估亚洲机构中接受根治性切除术的患者的临床结局、生存预后因素、复发模式和时间。
回顾性分析了 1998 年至 2013 年间接受根治性切除术的 165 例 PDAC 患者的临床病理和生存结局。手术时的中位年龄为 62.0 岁。55.2%为男性,73.3%的肿瘤位于胰头部。全队列的中位 OS 为 19.7 个月。接受辅助化疗的患者中位 OS 为 23.8 个月。生存的负预测因素包括淋巴结比率(LNR)>0.3(HR=3.36,P=.001)、肿瘤位于胰体或尾部(HR=1.59,P=.046)、存在神经周围侵犯(PNI)(HR=2.36,P=.018)和分化程度差/未分化肿瘤分级(HR=1.86,P=.058)。中位复发时间为 8.87 个月,12 个月和 24 个月时分别有 66.1%和 81.2%的患者复发。最常见的复发部位是肝脏。
接受辅助化疗的亚洲 PDAC 患者的生存与报告的随机试验相当。临床特征似乎与西方患者相似。因此,地理位置可能不是 RCT 中必要的分层因素。相反,淋巴结比率和 PNI 状态应该被纳入。